
Scenario: A provider organization has a value-based care agreement with a payer calling for improving the quality of care and patient satisfaction scores, and reducing cost among their shared population of patients/enrollees. While the contract lists performance indicators, both organizations have different perspectives regarding their responsibilities and implementation, and have data to measure performance against value-based care and population health goals. Each of them has better access to certain data and a different relationship with the population. How would they achieve their shared goals?
Several textbooks on population health (PH) exist, but there are few short practical guides on population health management (PHM) among the plethora of PH/PHM articles. This article presents an experience-informed, literature-supported outline for PHM programs. It describes the concept and its evolution and implementation, while highlighting contextual factors. Additional content, including healthcare trends, resource allocation, and impact evaluation can be found elsewhere.(1)
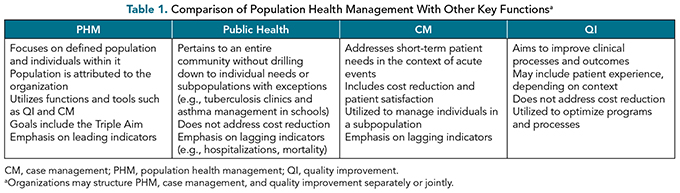
PHM and value-based care (VBC) share common goals of, at minimum, improving quality and reducing the cost of care. Adoption of VBC has varying results, depending on the complexity, experience, and other factors, usually with positive clinical and cost outcomes.(2) PHM is the strategy through which PH and VBC goals are achieved. It brings together other, closely related, concepts, including quality improvement, case management, disease prevention, and health promotion to improve population health outcomes (Table 1). Although small practices may not have PHM teams, the concepts discussed here would inform their involvement in government- and private-payer VBC models. PHM activities may serve as quality improvement projects, which would fulfill regulatory, accreditation, and recertification requirements for organizations and clinicians.
Definition of Population Health Management
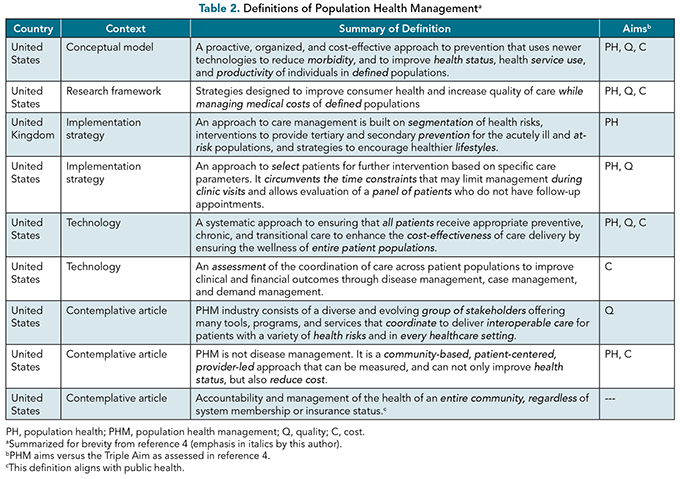
PHM focuses on improving the health of an attributable population, but definitions and perceptions have varied. A recent review of PH frameworks underscored this variability, in addition to a lack of metrics in about half of them, particularly older ones.(3) The theme of a discrete population is common among most definitions of PH/PHM, with differences discerned between them when they are examined through the Triple Aim lens (Table 2).(4) Some definitions emphasize medical aspects of the health of the population, whereas others include the physical and psychosocial well-being of its members. Data management, stratification, evaluation, and feedback cycles often are missing or only implied. One potential drawback of a focus on both a distinct population and specific measures is that the health of other individuals may be neglected; therefore, PHM programs and organizations should be mindful of other needs as well.
Public health, the last definition in Table 2, may be confused with PH/PHM. Conflating PHM and public health may confuse stakeholders about the role of providers, payers, and government agencies, and may misguide policymakers and funders, potentially resulting in budget and resource allocation concerns.(5)
Interest in PH, which is focused on improving the health of a population, grew in the 1990s, and it became a key element of the Triple Aim in 2008(6) (Figure 1). PHM is the strategy by which the Triple Aim concept is implemented to optimize the population’s health status, its experience of care (in terms of quality and satisfaction), and the cost of care (particularly avoidable ED and hospitalization costs). Both PHM and the Triple Aim call for specifying a population of concern, and both have evolved over time to encompass health equity and reducing healthcare disparities.(7) PHM definitions may not explicitly incorporate provider experience, which the Quadruple Aim has done so.(8) It is worth noting that VBC may increase the provider’s work burden and dissatisfaction.(2)
The definition of PH/PHM definition evolved as follows:(5-8)
Early conceptualization (pre-2008): Definitions were less comprehensive and were not explicitly linked to quality improvement and cost reduction.
The Triple Aim Era (2008 to the present): Because it was included in this framework, PH gained wider recognition; however, some definitions continued to lack one or more of the three aims.
Emergence of risk adjustment: Meaningful comparison of similar but separate populations, such as Medicare beneficiaries at various accountable care organizations and Medicare Advantage (MA) payers, relies on standardized measurement of disease burden (risk adjustment) in each group. PHM programs are increasingly managing initiatives to capture disease burden within their populations.
Focus on social determinants of health (SDOH): Definitions have increasingly encompassed SDoH with emphasis on integrating community and social services into PHM strategy. The COVID-19 pandemic highlighted significant health disparities among disadvantaged and minority groups, and strengthened the case for addressing SDoH and health inequity.
Emphasis on data and technology: Data management and analytics are integral to PHM to optimize decision making and allocation of scarce resources. The size and complexity of patient information have grown, and PHM utilizes increasingly sophisticated analytical techniques including machine learning.

Figure 1. The evolution of the Triple Aim. Adapted from references 6-8. *Scope per original description of
aims in reference 6.
Program Design
Given the varied definitions of PHM, individual PHM programs should include a definition in their charters to ensure that stakeholders are aligned regarding the scope and purpose of the program. The context of PH varies widely among organizations and influences how they support and utilize PHM.(5,9)
Effective PHM programs require careful design and implementation, particularly for organizations with significant revenues from VBC. They identify the target population and assess its current health status, experience of care, and utilization and cost of care to determine opportunities for improvement. Both program leadership and staff must communicate findings and recommendations with a diverse audience in mind. PHM teams should monitor and evaluate program effectiveness and then make changes to optimize their impact.
Data
Data play a vital role in PHM by furnishing insights that guide decision making, justify resource allocation, and evaluate impact. The requirements for PHM data are as follows:
Measure selection: Meaningful metrics measurement tools in the categories noted earlier are chosen according to the program’s goals and VBC terms.(6,10,11)
Sources: Measurement data are captured from patient and provider lists, claims, patient surveys, EMRs, various documents, health information exchanges, and public sources. It is essential to assess the quality of data in terms of veracity (accuracy), value, volume, velocity (frequency), variability and structure.
Integration and storage: Collating such diverse data is complex but provides a more comprehensive picture about the population, which would guide action planning. Data lakes support more complex forms of analysis and are more amenable to scaling, characteristics which large organizations may find attractive.
Analysis: The aim is to identify individuals who are at the highest risk of unfavorable cost or quality outcomes, and those with gaps in care. Although sophisticated analytical techniques, including machine learning,(12-14) are increasingly used to analyze PHM data, spreadsheet programs remain the workhorse of many PHM and finance teams.
Socialization: Summary findings and drilldown details are shared in different fashions depending on the audience (e.g., leaders versus support teams versus individual providers). The format, whether summary slides, dashboards, EMR alerts, etc., should be user friendly, and patient-level data such as care gaps should be easily accessible and addressable within EMRs rather than spreadsheet files.
Stratification
A key output of data analysis is risk stratification of the population, which segments it into meaningful subpopulations based on shared characteristics so that each subgroup would receive specified interventions, an approach that has yielded positive results (Figure 2).(14-16) Homegrown or commercial stratification scoring models are used identify the group(s) of higher-cost patients where interventions are likely to yield the most savings. Population segmentation yields risk scores, which may be derived from either simple scoring algorithms or complex predictive modeling.(12-14,17) The criteria and number of output strata vary among PHM programs, and the intensity of intervention increases for subpopulations with a higher likelihood of healthcare utilization, which often is associated with lower quality scores. Stratification design may combine subpopulations represented in Figure 2 such as merging “focus” and “high complexity,” or may split them — for example, subdividing “well” into “hidden risk” and “no risk”.

Figure 2. Example of population stratification. Dx, diagnosis; SNF, skilled nursing facility; Mgmt, management;
ER, emergency room; IP, inpatient; Rx, prescription(s).
Clinicians’ participation in designing and updating stratification models is important. Stratification criteria may include diagnoses, comorbidities and functional status, and demographic factors such as age, sex, and socioeconomic status. Specific diagnoses or events (e.g., end-stage renal disease) or a level of resource utilization such as superutilizers may define special subpopulations (indicated by “Focus” in Figure 2) and hierarchical condition categories (HCCs) may be used instead of or in addition to diagnoses. The resources available for the appropriate intervention for each subpopulation and their expected impact will be critical considerations in resource allocation and return-on-investment (ROI) analysis of existing and new initiatives.
Model outputs should be examined by clinicians for validity and utility, and stakeholders should ensure absence of bias in the model, to promote equity. PHM programs should coordinate with other teams that utilize purpose-specific identification tools — for example, the LACE Index for Readmission, which evaluates length of stay, acuity of admission, the presence of comorbid conditions, and recent emergency department use — to ensure alignment of efforts and to minimize provider and patient abrasion. New stratification models should be pre-evaluated because those developed for one population or setting may not apply to others. Existing models should be reviewed at least annually to update coding and clinical logic, align with regulatory or accreditation requirements, modify the associated interventions, and (re)allocate resources as needed.
Team Structure
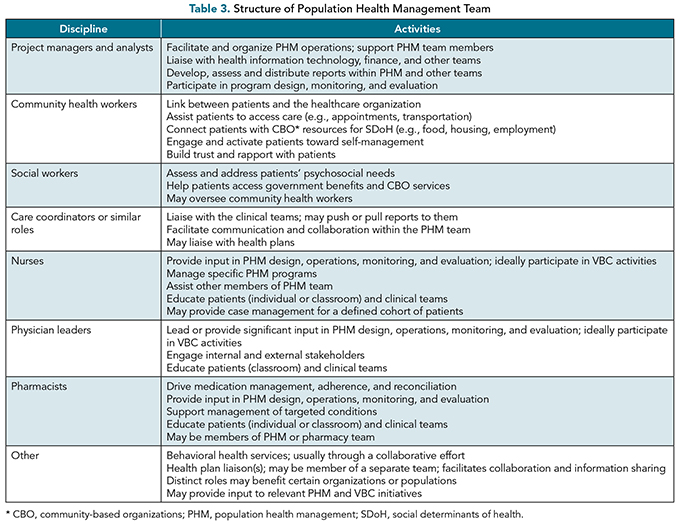
PHM teams are multidisciplinary because their planning and implementation require expertise from clinical and nonclinical disciplines to address the complex health needs of the population. Nontraditional staff increasingly are included in multidisciplinary PHM team and operations.(14,16) The team structure outlined in Table 3 varies considerably among organizations; some roles may reside in other departments, and some roles may change over time within the same department. Physician leaders play a crucial role in the successful design and implementation of PHM and VBC, and their contributions can serve organizations best through formal management of PHM teams rather than acting in a consultative capacity. They provide informed guidance and support for team members in addition to trusted accountability within and outside the organization. Their expertise and leadership are essential for achieving desired goals thanks to their ability to drive improvement in the face of a constantly changing environment and rising rates of clinician burnout.
Operations in Population Health Management
Several operational considerations in population health management require attention:
Clear roles and responsibilities that are consistent with the scope of practice for each team member;
Thorough and rational workflows that outline process steps within and outside the organization, taking into account uncommon scenarios;
Participatory input and a team-based approach that promotes a collaborative culture;
Evidence-based recommendations, interventions, policies, and procedures; and
Regular information sharing with clear protocols for communication within and outside the team, and receptiveness to feedback.
Detailed process descriptions such as “swim lane” workflows (Figure 3) delineate the responsibilities and accountability of each party. PHM operations entail regular meetings with various stakeholders to jointly share, discuss, update, plan, and facilitate activities. Periodic trend review by providers and payers is important, and may be held in one or more forums, such as joint (clinical) operational meetings and care management rounds.

Figure 3. Sample simplified “swim lane” workflow. Detailed workflows are designed and shared in a multidisciplinary fashion. Process and project managers facilitate the development of workflows. Org, organization. 1, Alternate processes may be intentional in some organizations; they may lead to confusion and inefficiency in others. 2, Protocols should include nursing review and decision making. 3, Workflows for patient recall, prescription refill, referral, and so on. PHM, population health management; VBC, value-based care.
Cost-optimization interventions may include complex case management for high-need/high-touch events and conditions; disease management for chronic conditions to curtail complications or exacerbations; care navigation to assist patients in accessing the right care at the right time in the right place; assessments of health, functional and/or disease status; and health education. Disease-specific interventions, community-based services,(14) home-based primary care,(19,20) and hospital-at-home programs(21) would benefit certain subgroups. Care and risk-adjustment gap closure activities (e.g., patient and provider reminders, reconciling gap lists with documentation in medical records, lab and specialist referrals) would apply to the entire population. Cyclical patterns, in which activities intensify during the year, may trigger different approaches, such as additional provider visits, at-home testing, or temporary staffing, among others. Recognizing those patterns and proactively planning for variable resource allocation optimize the impact of PHM.
Evaluation of the impact of PHM and the ROI from VBC agreements guides resource allocation, and value estimation of distinct interventions and the program relies on evidence-based knowledge and informed experience, both areas in which clinicians can provide important insights. Challenges in determining the value of PHM include annual variations, the length of time some outcomes may take to materialize, and the difficulty in attributing outcomes to specific interventions because of the complex interplay of factors and concurrent initiatives. Additional information regarding program evaluation and resource allocation is available elsewhere.(1)
Factors That Lead to Success
Organizations vested in VBC are more likely to develop and maintain strong PHM programs that are espoused as an enterprise-wide endeavor. Successful PHM programs share several characteristics related to their sponsorship, design, analytics, operations and interventions, as follows:
Alignment of PHM operations with contractual obligations to ensure that outcomes serve not only the patients but also organizational goals;
Close collaboration with the VBC team to align on the scope, selection, and number of measures for each contract, and the aggregate number of indicators across all payers;
Reliable data management and analytics that employ insightful segmentation models and adapt quickly to reporting requirements;
Robust, proactive rather than reactive, actions that take into account their target audience’s behavior patterns, and utilize continuous process improvement;
Effective and efficient interventions that address both preventable costs and the quality of care;
Flexible PHM designs that adapt to changes in the population, provider network, and regulatory and accreditation requirements;
Attention to communication, stakeholder buy-in, volume and format of data, clinician burnout, and staff roles throughout the organization;
Productive collaborations within and outside the organization to promote engagement and garner support, particularly during changing times;
Integration of various services including behavioral health, ideally co-located with primary care, and collaborations with community-based organizations; and
Understanding payer coverage and benefits that may impact beneficiary behaviors and utilization patterns, and potentially PHM effectiveness.
Summary
PHM programs aim to optimize, at minimum, the health status and quality and cost of care of attributable populations, which often are tied to VBC and are segmented to optimize the use and yield of resources. Successful PHM programs entail a wide range of activities, ideally addressing all aspects of the Quintuple Aim through effective communication, data management and reporting, broad collaboration, utilizing tools from other disciplines, and innovative nontraditional solutions. Concepts and models of PH and PHM will continue to change because of shifting population needs, economic and regulatory influences, mergers and acquisitions, evolving workforce, new technology, and other factors. Organizations and their various teams will need to adapt to those changes to maintain the impact and value of PHM.
References
Hakim A. Population health. Handel DA, ed. Healthcare Administration, Leadership, and Management (HALM): The Essentials First Edition. Washington, DC: American Association for Physician Leadership; 2025;81-92.
Pavlova M, Groot W. The Impact of value-based payment models for networks of care and transmural care: a systematic literature review. Appl Health Econ Health Policy. 2023;21:441-466. https://doi.org/10.1007/s40258-023-00790-z
Chan SL, Ho CZH, Khaing NEE, et al. Frameworks for measuring population health: a scoping review. PLoS ONE. 2024;19(2):e0278434. https://doi.org/10.1371/journal.pone.0278434
Steenkamer BM, Drewes HW, Heijink R, Baan CA, Struijs JN. Defining population health management: a scoping review of the literature. Popul Health Manag. 2017;20(1):74-85. https://doi.org/10.1089/pop.2015.0149
Noble DJ, Greenhalgh T, Casalino LP. Improving population health one person at a time? Accountable Care Organisations: perceptions of population health — a qualitative interview study. BMJ Open; 2014;4:e004665. https://doi.org/10.1136/bmjopen-2013-004665
Berwick DM, Nolan TW, Whittington J. The Triple Aim: care, health, and cost. Health Aff (Millwood). 2008;27:759-769. https://doi.org/10.1377/hlthaff.27.3.759
Olayiwola JN, Rastette M. Aiming for health equity: the bullseye of the Quadruple Aim. J Hosp Manag Health Policy. 2021;5:11. https://doi.org/10.21037/jhmhp-20-101
Bodenheimer T, Sinsky C. From Triple to Quadruple Aim: care of the patient requires care of the provider. Ann Fam Med. 2014; 12:573-576. https://doi.org/10.1370/afm.1713
Caldararo KL, Nash DB. Population health research: early description of the organizational shift toward population health management and defining a vision for leadership. College of Population Health Faculty Papers. 2017; Paper 79. https://jdc.jefferson.edu/healthpolicyfaculty/79 . Accessed September 16, 2024.
Stiefel M, Nolan K. A Guide to Measuring the Triple Aim: Population Health, Experience of Care, and Per Capita Cost. IHI Innovation Series white paper. Cambridge, MA: Institute for Healthcare Improvement. 2012. www.ihi.org/resources/white-papers/guide-measuring-triple-aim-population-health-experience-care-and-capita-cost . Accessed November 17, 2024.
Hendrikx RJP, Spreeuwenberg MD, Drewes HW, Ruwaard D, Baan CA. How to measure population health: an exploration toward an integration of valid and reliable instruments. Popul Health Manag. 2018;21:323-330. https://doi.org/10.1089/pop.2017.0097
Morgenstern JD, Buajitti E, O’Neill M, et al. Predicting population health with machine learning: a scoping review. BMJ Open. 2020;10:e037860. https://doi.org/10.1136/bmjopen-2020-037860
Li Z, Gogia S, Tatem KS, et al. Developing a model to predict high health care utilization among patients in a New York City safety net system. Med Care. 2023;61(2):102-108. https://doi.org/10.1097/MLR.0000000000001807
Baum A, Batniji R, Ratcliffe H, DeGosztonyi M, Basu S. Supporting rising-risk Medicaid Patients through early intervention. NEJM Catalyst. 2024;5(11):1-21. https://doi.org/10.1056/CAT.24.0060
Ziring J, Gogia S, Newton-Dame R, Singer J, Chokshi DA. An all-payer risk model for super-utilization in a large safety net system. J Gen Intern Med. 2018;33:596-598. https://doi.org/10.1007/s11606-018-4346-5
Soto-Gordoa M, de Manuel E, Fullaondo A, et al. Impact of stratification on the effectiveness of a comprehensive patient-centered strategy for multimorbid patients. Health Serv Res. 2019;54:466-473. https://doi.org/10.1111/1475-6773.13094
Wammes JJG, van der Wees PJ, Tanke MAC, et al. Systematic review of high-cost patients’ characteristics and healthcare utilisation. BMJ Open. 2018;8:e023113. https://doi.org/10.1136/bmjopen-2018-023113
Lammila-Escalera E, Greenfield G, Barber S, Nicholls D, Majeed A, Hayhoe BWJ. A systematic review of interventions that use multidisciplinary team meetings to manage multimorbidity in primary care. Int J Integr Care. 2022;22(4):6. https://doi.org/10.5334/ijic.6473
Edwards ST, Saha S, Prentice JC, Pizer SD. Preventing hospitalization with Veterans Affairs home-based primary care: which individuals benefit most? J Am Geriatr Soc. 2017;65:1676-1683. https://doi.org/10.1111/jgs.14843
De Jonge KE, Jamshed N, Gilden D, Kubisiak J, Bruce SR, Taler G. Effects of home-based primary care on Medicare costs in high-risk elders. J Am Geriatr Soc. 2014;62:1825-1831. https://doi.org/10.1111/jgs.12974
Shi C, Dumville J, Rubinstein F, et al. Inpatient-level care at home delivered by virtual wards and hospital at home: a systematic review and meta-analysis of complex interventions and their components. BMC Med. 2024;22,145. https://doi.org/10.1186/s12916-024-03312-3