
Communication among physicians, nurses, and other healthcare professionals is a critical determinant of healthcare outcomes.(1,2) While communication can be viewed as a simple transaction, clinicians converse in a multitude of diverse ways. For instance, nearly half of medical malpractice suits and many other adverse events involve communication errors.(3,4)
Clinician miscommunications can lead to serious medical errors, reduced patient satisfaction, poor patient outcomes, increased malpractice claims, and elevated burnout among healthcare professionals.(5)
Studies reveal that consistency in communication style across healthcare professionals improves the exchange of information.(6) Tools such as I-PASS (Illness severity, Patient summary, Action list, Situation awareness, and Synthesis by receiver) and SBAR (Situation, Background, Assessment, Recommendation) have streamlined communication in healthcare settings, thereby reducing adverse events.(7-10)
While these tools streamline structured exchanges, they cannot account for the more nuanced, interpersonal dynamics such as bias, tone, and emotional resonance. Clinicians bring their own life experiences and biases into every room they enter, affecting clinician-to-clinician and clinician-to-patient relationships and ultimately altering patient outcomes.
We propose that self-awareness, connection, and amplifying others’ successes are a critical foundation for effective communication in healthcare environments. These elements address the interpersonal and emotional context that current tools overlook, offering a more comprehensive approach to improving care coordination and outcomes. Without this foundational layer, structured communication efforts may remain technically sound but relationally insufficient.
ASPECTS OF EFFECTIVE TEAM COMMUNICATION
Promoting self-awareness and connection, and amplifying others’ successes can create a sturdy foundation of team communication into which more specific tools and strategies can be effectively integrated to improve patient care.
Self-Awareness
Self-awareness emphasizes introspection and supports authentic communication with others. When developing a culture of excellence in a healthcare setting, a keen sense of self can propagate outward, fostering a thriving healthcare team.
Self-awareness is essential given the emotional challenges inherent in healthcare environments. Clinicians are stressed by long hours, heavy workloads, competing priorities, and challenging patient conversations. Under such pressure, emotional regulation can influence decision-making, thereby affecting clinical leadership.(11)
Many clinicians react to these stressors with maladaptive coping responses such as emotional detachment (flight) or anger (fight); these professionals must recognize when this is occurring.(12) Such responses have been described as “going to the basement” or “amygdala hijack,” signifying an emotional state that does not contribute to productive interactions.(13) Promoting self-awareness and providing clinicians with the tools to recognize and reflect on their emotional dysregulation promotes the implementation of positive coping strategies.
In instances of disagreement among the healthcare team, self-aware clinicians advocate for their patients while simultaneously fostering a team culture of mutual respect and collegiality. Interpersonal conflict can trigger defensive responses that compromise both professional relationships and patient care.
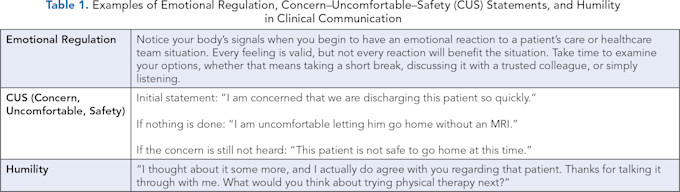
One method for navigating these difficult situations while maintaining both advocacy and authenticity is the CUS (Concern, Uncomfortable, and Safety) model. In practice, a provider describes what they are concerned about, what treatment they are uncomfortable with, and how they believe it negatively affects patient safety. This model has been used to promote patient safety by allowing clinicians to discuss treatment efficacy and outcome probabilities without escalating tensions.(14)
While the CUS method is helpful for speaking up, clinicians must balance assertiveness with humility, recognizing that acknowledging one’s fault is critical to team effectiveness. If clinicians incorporate humility into their practice, everyone is more willing to offer ideas without fear of retribution from their peers. This practice inherently promotes a more open environment with greater collaboration.
Ultimately, building a strong culture starts at an individual level through self-awareness, assertiveness, gratitude, and humility. Staying grounded in these ideals allows clinicians to respond genuinely rather than reactively, ensuring their true professional values guide their actions during high-stress situations.
Assertiveness empowers healthcare professionals to speak their truth, advocating honestly for patients and voicing legitimate concerns without hiding behind professional facades. Finally, humility encourages professionals to present themselves honestly, acknowledge their limitations, admit mistakes, and remain genuinely open to learning from others.
When practiced together, these qualities generate a comprehensive self-awareness that transcends individual interactions, creating a ripple effect throughout the healthcare environment. As each team member embodies this authentic approach, it influences colleagues to respond with similar genuineness and vulnerability, ultimately transforming the culture from defensive communication to collaborative excellence rooted in honest, compassionate care. Table 1 provides examples of emotional regulation, CUS statements, and humility in clinical communication.
Connection
Once providers have tapped into their self-awareness and are communicating with authenticity, they are better equipped to forge meaningful connections with their colleagues. By cultivating genuine relationships and learning from one another, clinicians can master the art of team building in any setting, deepening their understanding of those they work alongside.
Improving team connections starts by building rapport with colleagues through daily interactions. These connections often begin with small actions such as saying “hello,” calling people by their name, or checking in briefly between shared tasks. Subtle courtesies such as these may seem minor, but they establish micro connections that contribute to a more inviting work environment, allowing team members to feel seen and genuinely valued.
Over time, continued social interactions and relationship-building can help team members recognize when something in a colleague’s behavior seems unusual.(15) For these situations, adopting a trauma-informed mindset — understanding that colleagues may carry unseen burdens — can foster stronger relationships and more compassionate communications.(16) This approach requires withholding judgment and expressing empathy toward the team member. By shifting your mindset and listening attentively, you create an opportunity to have an open dialogue with your colleague and form a deeper connection. Practicing such an approach and expressing a compassionate tone de-escalates potential conflicts, builds trust, reduces error, encourages relationship building, and limits misunderstandings.(16)
For example, imagine you are a physician in a bustling pediatric clinic and notice that a normally composed nurse seems uncharacteristically flustered when asked, at the end of a long shift, to repeat vital signs for a patient. Instead of immediately thinking, “What’s wrong with that nurse?” a trauma-informed mindset encourages you to ask yourself, “What happened to our team member?” This reflective and intentional shift in language recognizes that behavioral changes often stem from underlying stressors or experiences rather than personal failings, acknowledging the nurse not just as a colleague, but as a valued member of the healthcare team. Adopting the report-building strategies outlined in Table 2 can address these circumstances.

Amplification
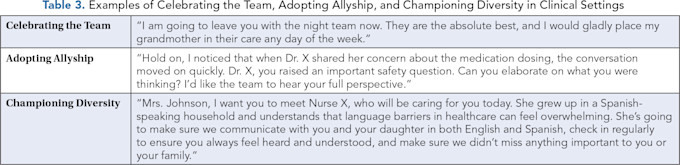
Amplification is a strategy teams often use to promote an atmosphere of camaraderie, trust, and cohesion. Publicly celebrating team wins and acknowledging others’ strengths ensures every team member feels valued in the presence of patients, peers, and leadership. Showcasing and celebrating team achievements instills individuals with a sense of confidence and belonging that is morale-boosting and emotionally protective.(17) Strategies that amplify team strengths include celebrating team wins in the presence of patients and family members and championing diversity within the team.
Publicly celebrating wins at both the team and individual levels helps foster a culture of solidarity and resilience in high-stakes healthcare environments plagued by burnout. A win for one is a win for all, and ultimately, a victory for the patient.(17) Whether it is a complex heart surgery or diligent neurological checks, the key is to acknowledge a job well done.(18) Many healthcare institutions have implemented strategies such as recognizing team members during huddles, which spark a ripple effect and boost the morale of the entire team.
One of the most critical aspects of maximizing the impact of team promotion is using language that highlights collective efforts rather than individual achievements.(19) This approach emphasizes the shared work of the healthcare team rather than personal accomplishments. Whether at the patient or leadership level, this strategy can be implemented by using inclusive language such as “together” or “our team” to convey unity and cohesion.(20) In fact, patients often view these phrases in a more positive light than terms that promote individual success.(20)
Another way to amplify the healthcare team is by championing diversity. Fostering a sense of belonging in the healthcare setting is a critical factor in optimizing patient care and cultivating an inclusive workplace.(19) It is not simply a buzzword that signifies racial representation; it encompasses differences in cultural background, personality, gender, and more. It is our individual differences that elevate team dynamics, not our similarities.(20) Team diversity improves communication, patient trust, team performance, patient safety, and outcomes.
Clinicians should adopt an attitude of allyship, ensuring that every team member feels respected and has a voice. Allyship involves aligning with colleagues from marginalized or underrepresented groups. Being an ally means speaking up when a colleague’s voice is minimized by better-represented members of the team. When team members champion belonging and inclusivity by using their status to amplify others, they help individuals feel supported and empowered.
This approach can be practiced in the clinical setting by speaking up when someone is exposed to microaggressions, bias, or being overlooked. This form of allyship creates a sense of safety in a group and highlights important differences without alienation or tokenism. Table 3 offers examples of celebrating the team, adopting allyship, and championing diversity in clinical settings.(21)
CONCLUSION
Supporting the healthcare team through self-awareness, connection, and amplification strategies can strengthen inter-professional communication and collaboration among providers. Practicing these skills in clinical settings helps foster a more cohesive, resilient, and effective care environment.(5)
Ultimately, our ability to communicate collaboratively within multidisciplinary teams will strengthen team dynamics, reduce burnout, elevate patient satisfaction, and improve patient outcomes.(1)
References
Zwarenstein M, Goldman J, Reeves S. Interprofessional collaboration: effects of practice-based interventions on professional practice and healthcare outcomes. Cochrane Database Syst Rev. 2009;(3):CD000072. https://doi.org/10.1002/14651858.cd000072.pub2 .
Rosenstein AH, O’Daniel M. A survey of the impact of disruptive behaviors and communication defects on patient safety. Jt Comm J Qual Patient Saf. 2008;34(8):464-471. https://doi.org/10.1016/S1553-7250(08)34058-6 .
Humphrey KE, Sundberg M, Milliren CE, Graham DA, Landrigan CP. Frequency and nature of communication and handoff failures in medical malpractice claims. J Patient Saf. 2022;18(2):130-137. https://doi.org/10.1097/PTS.0000000000000937 .
Shitu Z, Hassan I, Aung MMT, Tuan Kamaruzaman TH, Musa RM. Avoiding medication errors through effective communication in healthcare environments. Mov Health Exerc. 2018;7(1):113-126. https://doi.org/10.15282/mohe.v6i2.157 .
Green S, Markaki A, Baird J, Murray P, Edwards R. Addressing healthcare professional burnout: a quality improvement intervention. Worldviews Evid Based Nurs. 2020;17(3):213-220. https://doi.org/10.1111/wvn.12450 .
Johnson NL, Moeckli J. Conceptualizations of interprofessional communication in intensive care units: findings from a scoping review. J Commun Healthc. 2024;17(2):130-142. https://doi.org/10.1080/17538068.2023.2297124 .
Al-Hajjaji MSS, Imam AA, Hassan M, et al. Implementing electronic medical record (EMR) I-PASS–based handover: a method to improve the handoff process in an ACGME-I residency program. Pediatrics. 2021;147(3):10-12. https://doi.org/10.1542/peds.147.3MA1.10 .
Adam MH, Ali HA, Koko A, et al. The use of the situation, background, assessment, and recommendation (SBAR) form as a tool for handoff communication in the pediatrics department in a Sudanese teaching hospital. Cureus. 2022;14(11):e31998. https://doi.org/10.7759/cureus.31998 .
Starmer AJ, O’Toole JK, Rosenbluth G, et al. Development, implementation, and dissemination of the I-PASS handoff curriculum: a multisite educational intervention to improve patient handoffs. Acad Med. 2014;89(6):876-884. https://doi.org/10.1097/ACM.0000000000000264 .
Yun J, Lee YJ, Kang K, Park J. Effectiveness of SBAR-based simulation programs for nursing students: a systematic review. BMC Med Educ. 2023;23(1):507. https://doi.org/10.1186/s12909-023-04495-8 .
Liu B, Yang T, Xie W. Emotional regulation self-efficacy influences moral decision making: a non-cooperative game study of the new generation of employees. Int J Environ Res Public Health. 2022;19(23):16360. https://doi.org/10.3390/ijerph192316360 .
Gómez-Leal R, Gutiérrez-Cobo MJ, Megías-Robles A, Fernández-Berrocal P. The dark triad and subjective well-being: the mediating role of cognitive-emotional regulation strategies. Scand J Psychol. 2023;64(4):368-375. https://doi.org/10.1111/sjop.12890 .
Marcus LJ, Dorn BC, Henderson J, McNulty EJ. Meta-Leadership: A Framework for Building Leadership Effectiveness. Cambridge, MA: National Preparedness Leadership Initiative; 2015.
Puppala M, Ezeana CF, Alvarado MVY, et al. A multifaceted study of hospital variables and interventions to improve inpatient satisfaction in a multi-hospital system. Medicine (Baltimore). 2020;99(27):e23669. https://doi.org/10.1097/MD.0000000000023669 .
Edmondson A. Psychological safety and learning behavior in work teams. Adm Sci Q. 1999;44(2):350-383. https://doi.org/10.2307/2666999 .
Huo Y, Couzner L, Windsor T, et al. Barriers and enablers for the implementation of trauma-informed care in healthcare settings: a systematic review. Implement Sci Commun. 2023;4(1):49. https://doi.org/10.1186/s43058-023-00428-0 .
Sims S, Hewitt G, Harris R. Evidence of a shared purpose, critical reflection, innovation, and leadership in interprofessional healthcare teams: a realist synthesis. J Interprof Care. 2015;29(3):209-215. https://doi.org/10.3109/13561820.2014.941459 .
Amabile TM, Kramer SJ. The power of small wins. Harv Bus Rev. 2011;89(5):70-80.
O’Daniel M, Rosenstein AH. Professional communication and team collaboration. In: Hughes RG, ed. Patient Safety and Quality: An Evidence-Based Handbook for Nurses. Rockville, MD: Agency for Healthcare Research and Quality (US); 2008.
Carter BM, Johnson R, McDaniel VP, et al. The progression of inclusive language that enhances belonging. Creat Nurs. 2024;30(4):308-319. https://doi.org/10.1177/10784535241296824 .
Arif S, Afolabi T, Mitrzyk BM, et al. Engaging in authentic allyship as part of our professional development. Am J Pharm Educ. 2022;86(10):8690. https://doi.org/10.5688/ajpe8690 .