
Physician leadership is a key component of effective, efficient, innovative, and sustainable healthcare delivery in the United States. In the early 20th century, more than one-third of U.S. hospitals were physician-led,(1,2) a number that has dropped substantially to less than 6%.(1-4) Physician leadership in hospitals is associated with higher quality of care,(3,5-7) lower mortality rates,(8) greater inpatient bed utilization,(2,7,9,10) greater patient satisfaction,(8) and greater credibility among clinical staff and physician trust.(4)
While a 2009 study of top-ranked hospitals demonstrated an association between ranked quality measures and whether the chief executive officer (CEO) was a physician,(3) the claim that the CEO’s educational background has a significant impact on hospital safety and quality performance has not been strongly substantiated.(11-13) Rather, the presence of clinicians in key leadership and management positions in hospitals and healthcare organizations has a greater impact on financial and clinical performance.(11-14)
While formal training or a degree in business administration, management, and/or leadership may be important for hospital leaders, this training may provide little credibility in the absence of real-world experience or deference to those with such experience.(2) In many industries, working under a leader considered an expert in the organization’s core business is associated with higher employee job satisfaction and retention.(5) The healthcare sector is no exception, as more than one-quarter of health service managers believe that effective teamwork within the workplace is best fostered by leaders with high levels of clinical knowledge.(15)
Physicians are more likely to trust other physicians who have authentic clinical experience and are less likely to buy into patient-care decisions when they have not been involved in the decision-making process.(2,16,17) Visible physician representation benefits hospital performance and staff morale.
There is a growing interest in leadership development for physicians, fueled by increasing rates of burnout and decreased morale related to a lack of autonomy and self-governance.(1) The term “moral injury” has been proposed as a more accurate description of physician distress related to the challenge of knowing what patients need while simultaneously being unable to provide it.(18) The increasing complexity of the entire healthcare system contributes to moral injury by obfuscating delivery mechanisms of medical care with layers of additional process and policy. Hospitals can mitigate this by creating clarity within their own systems.
While each hospital system has its own distinct organizational structure, the Boston Children’s enterprise is particularly complex. The Children’s Medical Center Corporation (CMCC), a nonprofit 501(c)(3) organization, is the overarching corporate entity that controls entities within the system either directly or indirectly. These entities include, but are not limited to, The Children’s Hospital Corporation (Boston Children’s Hospital), 15 affiliated physician foundations, and the physicians’ organization (PO).
The PO at Children’s Hospital is a management service organization that supports the hospital and the foundations in developing and coordinating an integrated child healthcare system that fosters cost-effective, quality patient care. Most, but not all, clinical departments within Boston Children’s Hospital have a foundation that employs its physicians.
Foundations are separate nonprofit 501(c)(3) organizations that operate exclusively in support of the clinical, educational, research, and community missions of Boston Children’s Hospital and Harvard Medical School. Each faculty physician holds an academic appointment at Harvard Medical School, is an active member of Boston Children’s Hospital medical staff, and abides by medical school and hospital policies and procedures.
Boston Children’s Hospital appoints a chief for each of its major services, who also serves as president of the corresponding foundation. Each chief reports to the Boston Children’s Hospital executive vice president of health affairs. The layers of legal and financial complexity arising from these organizational relationships may lead to opaque processes for leadership and decision-making. Some physicians are unaware that the hospital is not their employer.
Boston Children’s Hospital has its own board, CEO, and president/chief operations officer (COO). Ten executive vice presidents (EVPs) answer to the CEO and COO; each oversees a different functional unit within the organization. There is overlap among EVP roles, which results in layered leadership. While redundancy safeguards against potential leadership gaps, it may inadvertently delay decision-making and/or dilute strategic input.
In the setting of such a complex decision-making apparatus, it is important for physician leaders to understand how to effect change within the hospital and identify opportunities for innovation and improvement. In this environment, a hospital-based physician leadership development curriculum designed to prepare future physician leaders to succeed within the current system (rather than leaving the organization) should be highly practical and bespoke to the institution.
At Boston Children’s Hospital, a cohort of mid-career faculty has been enrolling in leadership programs, earning business certifications and Master of Business Administration (MBA) degrees, signaling a desire to be involved in the management of the hospital. These physicians cite lack of access to or consideration for leadership opportunities as motivation to pursue additional training, particularly if they work within departments with limited advancement opportunities or if they have been passed over for opportunities by search processes that favor external candidates with administrative experience.
This lack of access to leadership opportunities is at least partly related to the complexity of the organizational structure. Many physicians are not aware of opportunities beyond those known to them within their individual departments, and/or may have a limited interprofessional network within the institution. Rather than lose valuable internal physician talent, Boston Children’s Hospital expanded potential opportunities for physician leaders by offering education, coaching, and mentorship from its own hospital leaders.
This program, known as the Emerging Physicians Leadership Program (EPLP), is geared toward physicians with business, leadership, and management training, equipping them with the requisite tools to optimize operations, improve collaborations among various hospital groups, and move into key leadership positions in hospital administration in the future. The unique curriculum is tailored to Boston Children’s Hospital, building upon a foundation of prerequisite leadership training and on-the-job experience, and applying the skills learned during training to the real-world management of the hospital.
The EPLP equips participants with institutional knowledge, expanded collaboration networks, and opportunities to demonstrate their leadership skills in a collaborative team-based environment. The goal of the program is to identify future hospital leaders and facilitate more seamless and successful transitions into hospital leadership roles. A secondary goal is to make the organizational structure and decision-making process more transparent and equip physicians with leadership potential to better integrate into and rise within the increasingly matrixed organization.
Emerging Physician Leadership Program at Boston Children’s Hospital
Establishing the Mission
Our mission was based on collective informal feedback from physicians as well as physician surveys. Many mid-career physicians felt removed from the decision-making process at the hospital, felt uninformed about decisions that affected them, and felt unempowered to impact administrative decision-making because of a lack of access to leadership. To address these important concerns, our mission had three main components:
To offer education, coaching, and mentoring in executive leadership for the next generation of physician leaders at Boston Children’s Hospital.
To consider leadership opportunities for physicians with appropriate training and experience.
To advise the current leadership of Boston Children’s Hospital on opportunities and barriers to the development and advancement of mid-career physicians.
Creating the Team
The executive vice president of health affairs, a practicing physician, served as executive sponsor for the project with the support of the CEO and executive leadership. Two physician faculty members with leadership experience and formal, graduate-level management training, both also mid-career faculty with many of the same characteristics as those for whom the program was being created, were selected to create and direct the program. A project manager was assigned to coordinate the program, and two administrative advisers were identified to help guide program development: a senior vice president and a senior director of professional medical staff services.
An oversight committee and an advisory board guide program development. The oversight committee consists of seven executive leaders in the hospital, including the chief medical officer, chief research officer, director of faculty development, director of education, chair of the medical staff executive committee, physician director of quality and safety, and a past department chief and leadership development expert. These individuals are responsible for selecting participants and contributing topics.
The advisory board consists of eight physician faculty members with executive leadership positions in addition to formal leadership and management degrees. All eight board members completed either a traditional or an executive MBA program. The advisory board members offer input into curriculum, speakers, and format, and are invited to attend sessions and contribute to the discussions. All members of the oversight committee and advisory board also volunteer to be coaches, sponsors, and mentors to the participants.
Call for Applications
The program enrolls a minimum of 12 and a maximum of 20 participants for each class. While relatively small, this size maintains the intimacy of a small group with opportunities for group work, executive coaching, and mentoring from hospital leaders.
The request for applications is distributed to all physicians through email, including all applicable listservs for various physician groups, and is posted on the hospital home page. Additionally, the program curriculum is presented annually at a meeting with department chiefs and physician faculty to broaden awareness and promote word-of-mouth marketing.
The request for applications calls for early- to mid-career physicians with either prior education in business/leadership (e.g., MBA or other leadership development program) or prior administrative/management experience. Sessions are scheduled once a month, and participants are asked to dedicate a maximum of five hours to the program between sessions. A letter from the department or division chief attesting that the participant will be given time to attend the sessions is required. Participants are offered a Certificate of Executive Leadership Training after completing the program.
A formal process is used to review and select applicants. Eligibility requirements are as follows:
Minimum of five years of experience as an active staff member at Boston Children’s Hospital.
Management or leadership experience in an administrative role (e.g., division chief, program director) and/or formal management/leadership training (e.g., MBA, executive MBA).
Participants require a letter of support from their department head as well as the names of two references who can attest to their leadership skills. The application includes a description of past and current leadership roles, and reasons for applying to the program. All materials are submitted with a copy of the applicant’s curriculum vitae. There is no cost to applicants, as the program is sponsored entirely by the hospital.
Selection Process
Each application is evaluated and scored independently by nine reviewers, including two program directors and seven members of the oversight committee. Each reviewer scores the applicant from 1 to 4 based on a global impression of the suitability of the applicant for a leadership role at Boston Children’s Hospital:
1 = Do not recommend
2 = Defer to future cycle
3 = Recommend
4 = Strongly recommend
The scores from all nine reviewers are summed into a total score, with nine representing the lowest possible score and 36 the highest possible score. Those with the highest scores are admitted to the program.
Content and Curriculum
The program is organized into 18 two-hour sessions scheduled once a month for nine months of the year (summers excluded). Individual session topics cover four major areas: 1) managing people, 2) financial management and strategy, 3) organizational structure and leadership, and 4) operations and research. There is a gradual and intentional progression of topics, with earlier sessions focused on organizational structure and dynamics unique to Boston Children’s Hospital, and later sessions emphasizing people management and strategy development (Table 1).
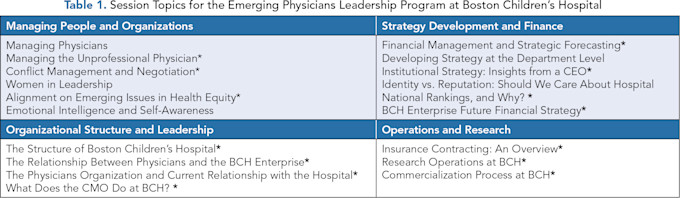
*Denotes topics that are tailored to Boston Children’s Hospital. Policies and processes presented may not apply to other organizations.
The sessions are a mix of didactic and discussion-based. Given that a prerequisite for selection into the program is previous formal leadership development or demonstrated leadership aptitude, the priority of EPLP is to refine and focus the training on the specifics of Boston Children’s Hospital. By doing so, the goal is to accelerate future onboarding for leadership positions by pre-emptively addressing institutional knowledge gaps. In addition, for several sessions, participants are asked to discuss specific, real-time challenges or questions they face and workshop them in small groups of 3–5 members.
In direct response to participant feedback from the initial program cohort, we added a speed-mentoring session, where participants rotate through stations where they speak briefly with potential faculty mentors who have agreed to be available to them throughout the program and beyond for career advice.
Faculty Mix
The decision to choose course faculty from within the institution is deliberate. EPLP is tailored specifically to the mechanics, structure, and organizational networks of Boston Children’s Hospital. The course faculty represents a mix of physicians and administrators with executive leadership roles in the institution. Course faculty members also serve as unofficial mentors and coaches for participants, alongside the advisory board and oversight committee members.
Faculty members include current and past CEOs, chief medical officers and associate chief medical officers, ombudsmen/women, chief administrative directors, chief financial officer, chief of staff, office of general counsel, chair of the advisory committee on professionalism and citizenship, prior and current department chiefs, innovation directors, chief scientific advisers, the director of pharmacy safety and quality, human resources directors, vice president of contracting, and chief operating officer of the physician’s organization, among others. We regularly amend and update the curriculum based on feedback and relevance.
Executive Coaching
Executive coaching is an essential tool in the professional development of physician leaders who will be called upon to transform workplace culture and improve engagement.(19) The program offers multiple opportunities for personalized leadership development and coaching.
An initial overview session is focused on leadership behaviors and common coaching areas for leaders, and the features of a personality profile assessment tool focused on emotional, relational, and team intelligence are reviewed. Each participant is encouraged to perform a psychometric assessment and personality test. Each participant is offered one-on-one development with a trained psychologist and the senior director of organizational development at Boston Children’s Hospital to review their profile and assess their leadership development needs.
Preparation Materials and Readings
Educational materials are provided to participants in advance of each session. Examples of readings include scientific articles, print material pertaining to management thinking, leadership challenges, financial concepts, and white papers related to Boston Children’s Hospital’s specific organizational structure.
In some instances, session leaders provide participants with pre-session questionnaires to better guide discussions around emotional intelligence, conflict management, and negotiation, as examples. The readings serve as brief introductions to relevant topics.
Program Evaluation Metrics
After each session, each participant receives an anonymous electronic feedback form and is asked to rate the format, topic, and speakers on a 5-point Likert scale from very unsatisfactory to very satisfactory. Free text fields include “What did you like most about this session?” “What did you like least about the session?” and “How could we improve this session in the future?”
An informal feedback session takes place halfway through the program, where participants discuss and share any positive or negative feedback about the program, as well as make recommendations for future sessions.
Lastly, each participant is asked to complete a comprehensive program evaluation at the end of the two-year curriculum, rating all individual sessions on overall value, relevance to their career, and quality of speakers. Twelve additional questions determine how well the EPLP has prepared them for leadership roles at the hospital (Table 2). This feedback is used to adjust and plan future sessions.
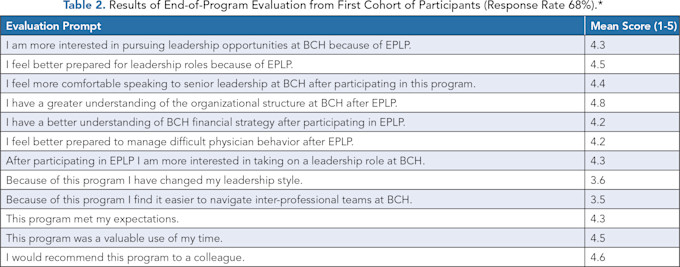
*Respondents were asked to respond to each question on a 5-point scale ranging from strongly disagree (1) to strongly agree (5). BCH = Boston Children’s Hospital.
Discussion
As hospitals and healthcare systems become more complex, the administrative apparatus required to support them must also expand. In a time of physician shortages, administrative leadership roles are progressively filled by non-MD executives, which may widen real or perceived gaps between physicians and hospital decision-makers.
Shifting hospital management roles away from physicians may reduce the impact of clinical insights on operational processes and lead to diminishing morale. Promoting physicians into administrative leadership positions may result in more efficient clinical operations, particularly if physicians are trained in effective leadership strategies.(5) Hospitals may find that decisions are achieved more readily and buy-in is achieved more easily with physicians at the table. A focused leadership development program tailored to the organization in which those physicians work has the potential to place those with the desire and ability to lead in the position to do so most effectively.
An increasing number of physicians work as employees in large healthcare systems or in multispecialty groups or practices with little control over their work environment or expectations. This loss of autonomy and lack of input into hospital decision-making was one reason nearly 300 primary care physicians at Mass General Brigham petitioned the National Labor Relations Board in 2024 to unionize.(20) Those in favor of increased physician leadership in hospitals cite improved patient outcomes, resource allocation, and service as motivating factors.(21,22)
Physicians often lack formal business training and have little experience managing people and projects.(23) Core knowledge requirements for physician leaders include finance, microeconomics, organizational design, health law, marketing, basic accounting, and strategic planning,(21,23) as well as organizational behavior skills, including motivation, communication, team-building, conflict management, and analytical skills.(24)
Several dual-degree MD-MBA programs have been developed in addition to traditional MBA programs.(25) The option of more focused executive MBA programs is desirable for physicians,(26) including programs focused exclusively on the healthcare sector.(27,28) Anecdotally, many physicians who have successfully completed an MBA or executive-MBA program report that skills gained in these programs did not help them navigate the complex environment in which they work. Most returned to their former roles after their program without putting newly attained skills into practice.
A survey of 104 healthcare systems revealed that 53 of these systems reported some form of established executive leadership development program, and 12 had a program under development.(29) An important outcome for physician leadership programs is to provide participants with an enhanced understanding of one’s own organizational structure,(30) although most physician leadership programs train core leadership competencies.
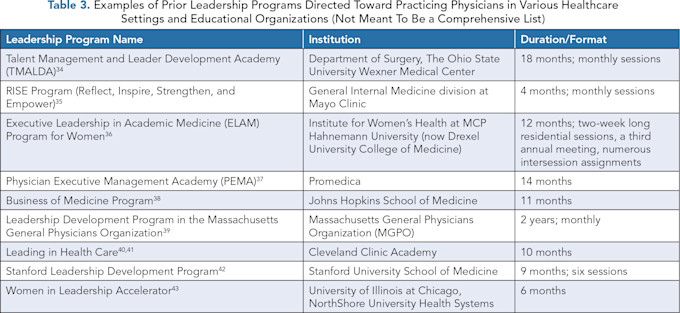
Several hospitals or departments within hospitals have successfully initiated leadership development programs tailored for practicing physicians (see Table 3 for examples). A systematic review of leadership development programs for physicians indicates they are associated with increased self-assessed knowledge and expertise, although few studies have measurable objective outcomes.(31)
EPLP was first officially offered at Boston Children’s Hospital as a two-year certificate program in 2022. It received 57 applications across 11 hospital departments. Given the strong interest in the program, the top 20 candidates were accepted based on summative scores. Of the 20 selected candidates, the following departments were represented: pediatrics (12, spanning eight divisions), anesthesia (3), neurology (2), neurosurgery (1), orthopaedic surgery (1), and cardiology (1).
Females represented 65% of the accepted cohort. Accepted applicants had been faculty members at BCH for a mean of 14.75 years (range 4–19 years). Out of the 20 accepted applicants, seven had previously obtained a Master of Public Health (MPH), one had completed an MBA program, two had completed executive-MBA programs, nine had completed a dedicated leadership training program, and two had completed masters-level programs in education and clinical investigation, respectively. The majority currently held an administrative position within their clinical department (director of a clinical or education program, division chief, or vice-chair), and one served as an associate chief for a hospital service.
As demonstrated in a post-program survey, graduates from the first cohort of EPLP felt better prepared and more interested in pursuing leadership roles at the hospital after participating in the program (Table 2). Many endorsed a greater understanding of the organizational structure of the institution and were more comfortable speaking to senior leadership after going through the program (Table 2).
Although it is impossible to prove that EPLP was directly or causally related to any subsequent leadership promotions, within one year of completing the program, seven of the initial 20 EPLP participants were promoted into a higher leadership role, including division chief (4), vice-chair within their department (1), and senior director of hospital programs (2). Although these individuals were already on track for professional advancement before enrolling in EPLP, given their exemplary qualifications and experience, our survey data indicate that participants were more prepared and more interested in pursuing these opportunities after completing the program.
Conclusion
The Emerging Physicians Leadership Program is a unique program developed at Boston Children’s Hospital that provides highly relevant and tailored institutional learning to physicians identified as future leaders by those currently in executive leadership roles. As hospital systems and organizational matrix structures become increasingly complex, this type of bespoke leadership development program is considered vital to the future success of the enterprise.
Creating robust interprofessional networks and reinforcing effective organizational collaborations improves institutional culture, strengthens engagement in quality improvement efforts,(32) and improves physician wellness.(33) The EPLP creates an internal pipeline of future leaders for our organization, as physicians who feel valued by an organization that invests in their professional growth are more likely to reciprocate this favor by assuming leadership roles.(32)
The EPLP has successfully concluded one full cycle and is currently in its second iteration. Our next goal will be to measure the success of the program in terms of mid- and long-term participant and institutional outcomes. While 35% (7 out of 20) of early participants were promoted into more senior leadership roles within one year of completing the program, future investigation will aim to assess how EPLP contributed to their success in these roles.
We predict physician leaders will have a more immediate impact in new leadership roles after completing EPLP, with less time spent onboarding and a greater ability to influence change by leveraging institutional knowledge and connections. This stands to benefit not only the individual, but also the hospital and all those working under these newly empowered leaders.
Acknowledgments: We would like to thank attorney Erica Carroll for her assistance in drafting the discussion pertaining to the organizational structure at Boston Children’s Hospital. We also thank Jane Choura for her assistance with manuscript preparation.
References
Gunderman R, Kanter SL. Perspective: Educating physicians to lead hospitals. Acad Med. 2009;84(10):1348–1351. https://doi.org/10.1097/acm.0b013e3181b6eb42 .
Falcone RE, Satiani B. Physician as hospital chief executive officer. Vasc Endovascular Surg. 2008;42(1):88–94. https://doi.org/10.1177/1538574407309320 .
Goodall AH. Physician-leaders and hospital performance: is there an association? Soc Sci Med. 2011;73(4):535–539. https://doi.org/10.1016/j.socscimed.2011.06.025 .
Gupta A. Physician versus non-physician CEOs: The effect of a leader’s professional background on the quality of hospital management and health care. J Hosp Adm. 2019;8(5):47–51. https://doi.org/10.5430/jha.v8n5p47
Stoller JK, Goodall A, Baker A. Why the best hospitals are managed by doctors. Harvard Business Review. December 27, 2016. https://hbr.org/2016/12/why-the-best-hospitals-are-managed-by-doctors .
Jiang HJ, Lockee C, Bass K, Fraser I. Board oversight of quality: any differences in process of care and mortality? J Healthc Manag. 2009;54:1.
Belasen A, Belasen A, Feng Z. The physician CEO advantage and hospital performance during the COVID-19 pandemic: capacity utilization and patient satisfaction. J Health Organ Manag. Published online March 3, 2023. https://doi.org/10.1108/jhom-04-2022-0126
Kaiser F, Schmid A, Schlüchtermann J. Physician-leaders and hospital performance revisited. Soc Sci Med. 2020;249:112831. https://doi.org/10.1016/j.socscimed.2020.112831 .
Tasi MC, Keswani A, Bozic KJ. Does physician leadership affect hospital quality, operational efficiency, and financial performance? Health Care Manage Rev. 2019;44(3):256–262. https://doi.org/10.1097/hmr.0000000000000173 .
Perry J, Mobley F, Brubaker M. Most doctors have little or no management training, and that’s a problem. Harvard Business Review. December 15, 2017. https://hbr.org/2017/12/most-doctors-have-little-or-no-management-training-and-thats-a-problem .
Razick DI, Monroe R, Sario E-M, et al. Does the chief executive officer (CEO)’s educational background have an impact on the academic hospital Leapfrog safety grades? Cureus. 2024;16(7):e64033. https://doi.org/10.7759/cureus.64033 .
See H, Shreve L, Hartzell S, Daniel S, Slonim AD. Comparison of quality measures from US hospitals with physician vs nonphysician chief executive officers. JAMA Netw Open. 2022;5(10):e2236621. https://doi.org/10.1001/jamanetworkopen.2022.36621 .
Moores LE, Landry A, Hernandez SR, Szychowski JM, Borkowswi N. Reported clinical and financial performance of hospitals with physician CEOs compared to those with nonphysician CEOs. J Healthc Manag. 2021;66(6):433–448. https://doi.org/10.1097/jhm-d-20-00157 .
Sarto F, Veronesi G. Clinical leadership and hospital performance: assessing the evidence base. BMC Health Serv Res. 2016;16(Suppl 2):169. https://doi.org/10.1186/s12913-016-1395-5 .
Leggat SG. Effective healthcare teams require effective team members: defining teamwork competencies. BMC Health Serv Res. 2007;7:17. https://doi.org/10.1186/1472-6963-7-17 .
Bailey-Wheaton J, Zigrang TA. Hospitalist pilot model sparks controversy. Chicago Medicine. May 2019.
Darzi A. A time for revolutions—the role of clinicians in health care reform. N Engl J Med. 2009;361(6):e8. https://doi.org/10.1056/nejmp0905707 .
Dean W, Talbot S, Dean A. Reframing clinician distress: moral injury not burnout. Fed Pract. 2019;36(9):400-402. Erratum in: Fed Pract. 2019;36(10):447. https://pmc.ncbi.nlm.nih.gov/articles/PMC6752815/ .
Kirk VG, Kania-Richmond A, Chaput K. Executive coaching for leadership development: experience of academic physician leaders. Healthc Q. 2019;22(1):54–59. https://doi.org/10.12927/hcq.2019.25835 .
Saltzman J. ‘Very new’: Doctors are unionizing, from Mass General Brigham to Beth Israel. Here’s why. Boston Globe. January 2, 2025.
Zismer DK, Flygenring B, Campion B. Physician-led: good idea or not? Physician Exec. 2002;28(5):20–23.
Butcher L. Physician leaders lower costs through care redesign. Physician Exec. 2014;40:14–18. PMID: 25188973.
Wain MJ, Handel DA, Williford K, Stewart KE. Transitioning from physician to hospital leader: a competency-based model. Physician Leadersh J. 2020;32.
Chaudry J, Jain A, McKenzie S, Schwartz RW. Physician leadership: the competencies of change. J Surg Educ. 2008;65(3):213–220. https://doi.org/10.1016/j.jsurg.2007.11.014 .
Turner AD, Stawicki SP, Guo WA. Competitive advantage of MBA for physician executives: a systematic literature review. World J Surg. 2018;42(6):1655–1665. https://doi.org/10.1007/s00268-017-4370-3 .
Lee CS, Ooi ASH, Zenn MR, Song DH. The utility of a master of business administration degree in plastic surgery: determining motivations and outcomes of a formal business education among plastic surgeons. Plast Reconstr Surg Glob Open. 2018;6(6):e1796. https://doi.org/10.1097/gox.0000000000001796 .
Lazarus A. Physicians with MBA degrees: change agents for healthcare improvement. J Med Pract Manage. 2010;26:188–190. PMID: 21243893.
Stahl MJ. The future of physician leadership education: customer value and technology in PEMBA (Physician Executive MBA). J Oncol Manag. 1999;8(1):21–22.
McAlearney AS. Executive leadership development in U.S. health systems. J Healthc Manag. 2010;55(3):206–222. PMID: 20565036.
Gabel S. Expanding the scope of leadership training in medicine. Acad Med. 2014;89(6):848–852. https://doi.org/10.1097/acm.0000000000000236 .
Frich JC, Brewster AL, Cherlin EJ, Bradley EH. Leadership development programs for physicians: a systematic review. J Gen Intern Med. 2015;30(5):656–674. https://doi.org/10.1007/s11606-014-3141-1 .
Debets M, Jansen I, Lombarts K, et al. Linking leadership development programs for physicians with organization-level outcomes: a realist review. BMC Health Serv Res. 2023;23(1):783. https://doi.org/10.1186/s12913-023-09811-y .
Khan TW. Improving wellness by improving autonomy through physician leadership development. Acad Med. 2017;92(7):895. https://doi.org/10.1097/acm.0000000000001739 .
Satiani B, Sena J, Ruberg R, Ellison EC. Talent management and physician leadership training is essential for preparing tomorrow’s physician leaders. J Vasc Surg. 2014;59(2):542–546. https://doi.org/10.1016/j.jvs.2013.10.074 .
Bhagra A, Croghan IT, Monson TR, Schletty AA, Badeke LK, Ghosh K. An innovative, pilot program to enhance career development and staff engagement for mid- and late-career physician staff within an academic institution: the RISE program. Mayo Clin Proc Innov Qual Outcomes. 2020;4(6):786–791. https://doi.org/10.1016/j.mayocpiqo.2020.07.016 .
Richman RC, Morahan PS, Cohen DW, McDade SA. Advancing women and closing the leadership gap: the Executive Leadership in Academic Medicine (ELAM) program experience. J Womens Health Gend Based Med. 2001;10:271–277. https://doi.org/10.1089/152460901300140022 .
Oostra RD. Physician leadership: a central strategy to transforming healthcare. Front Health Serv Manage. 2016;32:15–26. PMID: 27125046.
Cunningham TT 3rd. Developing physician leaders in today’s hospitals. Front Health Serv Manage. 1999;15:42–44. PMID: 10387766.
Gagliano NJ, Ferris T, Colton D, Dubitzky A, Hefferman J, Torchiana D. A physician leadership development program at an academic medical center. Qual Manag Health Care. 2010;19:231–238. https://doi.org/10.1097/qmh.0b013e3181eb13ab .
Stoller JK, Berkowitz E, Bailin PL. Physician management and leadership education at the Cleveland Clinic Foundation: program impact and experience over 14 years. J Med Pract Manage. 2007;22(4):237–242. PMID: 17425027.
Stoller JK. Commentary: Recommendations and remaining questions for health care leadership training programs. Acad Med. 2013;88(1):12–15. https://doi.org/10.1097/acm.0b013e318276bff1 .
Hopkins J, Fassiotto M, Ku MC, Mammo D, Valantine H. Designing a physician leadership development program based on effective models of physician education. Health Care Manage Rev. 2018;43(4):293–302. https://doi.org/10.1097/hmr.0000000000000146 .
Himstedt JDS, Bloomgarden E, Shah P. Empowering the invisible: accelerating leadership development for midcareer women in medicine. J Med Internet Res. 2023;25:e47801. https://doi.org/10.2196/47801 .