
It is difficult to accurately measure the prevalence and incidence of sexual misconduct and harassment because of underreporting or unreported events; however, numerous surveys from research projects, the popular press, and retrospective analysis of reports from the Equal Employment Opportunity Commission (EEOC) indicate the continued high incidence of the behaviors.
The April 2022 EEOC Data Highlight reported that between 2018 and 2021, 78% of sexual harassment charges were filed by women. These data are consistent with numerous validated surveys finding that women remain the primary target for sexual harassment and related behaviors.(1)
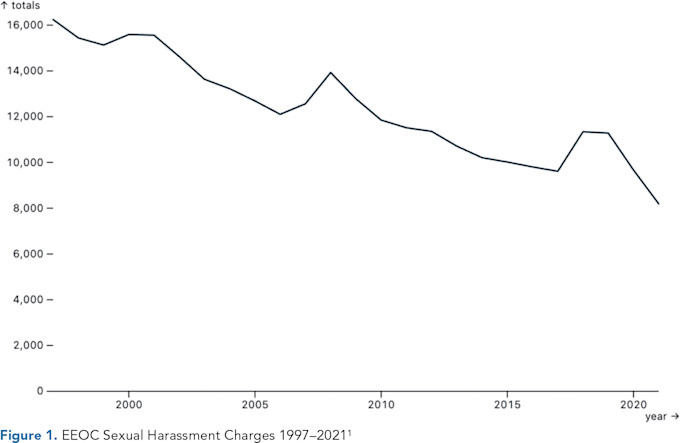
Since the late 1990s, the number of charges has slowly decreased except for a brief uptick in the number of charges from 2017 to 2020 corresponding to increased awareness from the #MeToo movement.
As shown in Figure 1, the number of charges continues to decline but remains unacceptably high. Thousands of charges are filed annually, and these charges represent a fraction of the total number of charges that could be filed. Fear of retaliation and retribution remains an obstacle and is discussed in greater detail in the chapter on barriers to reporting.
A factor contributing to the decline in the number of reported cases is greater awareness of the problem and, I surmise, the establishment of better processes within organizations to internally manage and respond to allegations and reports promptly — thus negating the need to turn to the EEOC.
In many healthcare organizations, anonymous reporting systems have been created to not only report patient safety concerns, but also professionalism issues and all other types of harassment behaviors, including sexual harassment. These anonymous reporting systems allow organizations to quickly identify and promptly respond to concerns and take a proactive, not reactive response.
SEXUAL HARASSMENT IN THE HEALTHCARE SETTING
Nurses provide most of the bedside care, and the frequency and duration of contact with patients and with other nurse colleagues on the wards creates an environment for higher rates of sexual harassment and misconduct. In the United Kingdom, where 86% of nurses are female and 14% are male, 60% of nurses say they have experienced sexual harassment at work. Importantly, only 27% of them reported it to their employer.
In addition, 39% of nurses say they have witnessed a colleague being harassed at work, 56% of nurses report verbal harassment, 37% report physical harassment, and 29% experience visual harassment, and 58% of nurses have been harassed by a patient. What’s more, 26% of nurses are harassed by medical colleagues and 24% are harassed by nursing colleagues.(2)
Clearly, the prevalence and incidence of these behaviors in healthcare are unacceptably high.(2)
An article by Choo, van Dis, and Kass published in The New England Journal of Medicine in 2018, reported that nearly 50% of female medical students will experience sexual harassment by the time they finish medical school.(3) This is unacceptable, and effective interventions to reduce the incidence are necessary.
The number of women in the physician workforce has been rising for decades. In 1980, 25% of medical school graduates were women. As of 2021, 37% of active physicians in the United States are women. And as of 2019, 47% of residents and fellows in post-graduate training programs were women.(3)
A 2018 Medscape survey revealed that 28% of physicians experienced sexual harassment by patients.(4) In 2018, the specialty of dermatology had the dubious distinction of being the specialty with the highest rate of sexual harassment by patients at 46%. A factor contributing to this may be that dermatologists must perform a full head-to-toe physical exam for screening of skin lesions and abnormalities.
Notably, 40% of male providers in a 2020 University of Washington survey of the Department of Dermatology reported sexual harassment.(5) Specific behaviors reported included comments on appearance (85%), questions about marital status (59%), jokes or stories of a sexual nature (35%) and being asked on a date (11%). Veterans Affairs outpatient clinics had the highest reported frequency of sexual harassment from patients, followed by outpatient academic clinics.(5)
In a 2019 Massachusetts study of resident physicians, 61% of participants reported personal experience with gender-based bias or discrimination during residency, including 93% of women and 24% of men. Sexual harassment was experienced by one-third of women. Only 5% of women formally reported these events.(6) Barriers to reporting included fear of retaliation, humiliation, and damage to one’s career and reputation.(7)
CREATING A SAFE CULTURE
The data and research reveal continued widespread prevalence and incidence of both discrimination and harassment. A strategy to continue to make efforts to reduce the behaviors includes developing systems and processes that break down the barriers to reporting. Creating a safe culture without fear takes time and requires employers, schools, and training programs to create a safe environment where employees, students, and residents feel protected and validated to report an incident or concern.
Excerpted from Sexual Misconduct, Harassment, and Discrimination in Healthcare: History, Analysis, and Solutions with Case Studies by Matthew J. Mazurek, MD, MBA, MHA, CPE, FAAPL, FACHE, FASA.
References
Equal Opportunity Employment Commission. Sexual-Harassment-Based Charge Data. Accessed March 25, 2024. https://www.eeoc.gov/sites/default/files/2021-12/Sexual%20Harassment%20Charges_FY2020_0.pdf .
Mitchell G. Exclusive: Survey Reveals a Majority of Nurses Have Experienced Sexual Harassment. Nursing Times. June 3, 2021. Accessed March 23, 2024. https://www.nursingtimes.net/news/workforce/exclusive-survey-reveals-majority-of-nurses-have-experienced-sexual-harassment-03-06-2021/ .
Choo E, van Dis J, Kass D. Perspective: Time’s Up for Medicine? Only Time Will Tell. N Engl J Med. 2018;379(17):1592–1593. https://doi.org/10.1056/NEJMp1809351
Kane L. Sexual Harassment of Physicians: Medscape 2018 Report. June 13, 2018. Accessed April 2, 2204. https://www.medscape.com/slideshow/sexual-harassment-of-physicians-6010304?icd=login_success_email_match_norm .
Notaro E, Pascoe V, Shinohara MM, DeNiro K. Sexual Harassment from Patient to Provider. Int J Womens Dermatol. 2019;6(1):30–31. https://doi.org/10.1016/j.ijwd.2019.09.001
McKinley S, Wang L, Gartland R, et. al. “Yes, I’m the Doctor”: One Department’s Approach to Assessing and Addressing Gender-Based Discrimination in the Modern Medical Training Era. Acad Med. 2019;9(11):1691–1698. https://doi.org/10.1097/ACM.0000000000002845
Cortina L, Berdahl J. Sexual Harassment in Organizations: A Decade of Research in Review. In: The SAGE Handbook of Organizational Behavior: Volume 1 – Micro Approaches, Barling J, Cooper CL, eds. SAGE Publications Ltd; 2008: 26, 469–497. https://doi.org/10.4135/9781849200448.n26