New Economic Pressures on U.S. Hospitals
The healthcare system in the United States, espoused for incredible advances in care, also receives tremendous criticism for its unsustainable high costs to all stakeholders, as well as its complicated and fragmented models of care. The COVID-19 pandemic exposed nearly all of the flaws of this system, and U.S. healthcare now finds itself struggling to manage its operational costs amid unprecedented inflationary pressures. The rise in labor costs and ongoing disruptions in healthcare supply chains (e.g., medications, IV contrast media, medical devices) will not deflate in the near term. Hospitals are continuously adjusting budgets, leading to downward margin projections at a rapid pace. Added to these pressures are downward equity markets, increased borrowing costs, and market share losses, along with digital disruptors and regional competition, so it is a wonder that more hospitals don’t announce insolvency. Fortunately, according to Kaufman Hall’s latest reports, there are some signs of stabilization ahead, but community hospitals must continue to develop models of sustainability.(1)
In the face of such pressures, it is worth pointing out that at the core of an acute care facility (i.e., hospital), revenue is generated by the activities of its providers, primarily its physicians. Most, if not all, of the profitable enterprise of a hospital occurs by either the direct hand(s) of a skilled practitioner in the operating room, cardiac catheterization lab, or other procedural areas, or by experienced management of the patient length of stay balanced with the diagnosis-related group–based prospective payment. Some hospitals benefit from revenue from outpatient diagnostic services (e.g., laboratory and imaging studies) or from lower cost structures (e.g., 340b Drug Pricing Program), but those dollars are also fundamentally the result of a doctor’s order. And although emergency departments also generate dollars from various activities, again the two primary emergency department events—treat and release or admission of patients—are dictated by provider decision-making. It should be noted that, generally speaking, emergency services remain depressed from pre-pandemic levels, a volume loss that only adds to the balance sheet woes of hospitals. According to the American Hospital Association, there are 6093 hospitals in the United States, with most of them—5139— existing as community-based institutions (urban/rural). The economic pressure on this national critical infrastructure is no small issue.(2)
Physicians as Key Drivers of Sustainability
What is missing from most headlines and tabletop discussions is the role that physicians will play in helping to right the “hospital ship” in the months and years ahead, and, most importantly, the role that physicians will (and must) play in the sustainability of acute care facilities in the United States in the coming decade. If the social desire (and political will) is to maintain the current system, for all its faults, for the immediate and foreseeable future, hospitals need to continue to deepen their relationships with their medical staffs and explore novel ways of creating sustainable partnerships with them.
Typically, employed physicians (and, to some degree, contracted physicians) are seen as cost centers relative to health system financial reviews. Although those same providers generate (or manage) the desired revenue in the hospital ecosystem, it is uncommon to account for that revenue as a net. Rather, the daily cash/accrual accounting practices are simply that, and physician labor remains as a separate line item in the system accounting. To reduce such cost, physician employment contracts simply could be terminated with the hope that every terminated employed physician would remain in place and would still be as productive as ever. As most operator administrators know, however, this is highly unlikely, and the loss of downstream revenue to the economic engine of the hospital would not be trivial. Anyone who has ever separated from a physician and/or group of physicians has lived through the financial impact, both immediate and beyond. Physician labor costs also are framed as “subsidy,” because their professional billings alone, once overhead is expensed, rarely can cover the salary or productivity structure.
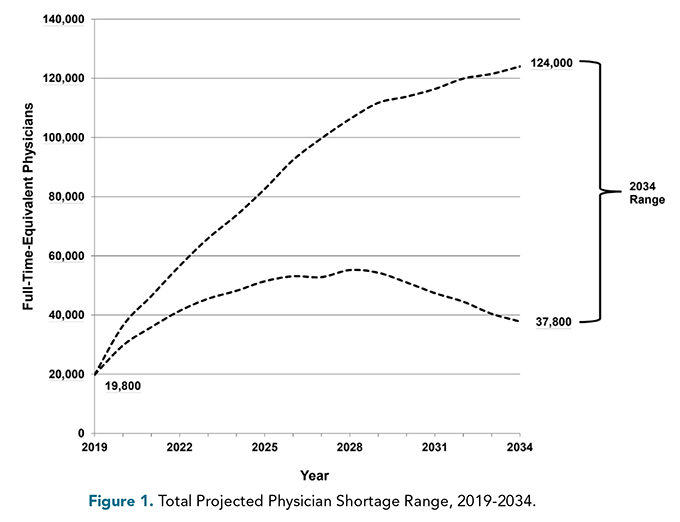
As a function of operations, therefore, hospitals with employed or contracted physicians continuously monitor all of their revenue, including technical and facility revenue and DRG payments, and hope to forecast that the net revenue can cover the subsidy and still provide a contribution to the hospital’s profit margin. Similarly, when physicians’ contracts are terminated or physicians leave because of illness, retirement, or death (117,000 physicians left their roles last year)(3), there is a net loss to the facility, and recruitment, replacement, and retention traditionally come at a very high cost. Hospitals with high physician attrition will bear a burden that has a pronounced ripple effect on the profit and loss results. A factor that is especially alarming for the future of hospitals is the growing shortage of physicians. Several years ago, it was projected that under the “best worst case” scenario there would be a shortage of approximately 37,800 while the “worst worst case” shortage was estimated to reach 124,000 by 2034 (Figure 1).(4)
Across the United States, large nonacademic hospital systems have embraced the integration of both undergraduate and graduate medical education over the years.
Florida, where this writer resides, faces a disproportionate shortage as it continues to grow rapidly. After decades of rapid population increase, Florida now is the nation’s fastest-growing state, with slightly more than 700,000 new residents between 2020 and 2022 according to the U.S. Census Bureau.(5) Florida will be short almost 18,000 physicians by the year 2035, according to the Safety Net Hospital Alliance of Florida and the Florida Hospital Association, an advocacy group for more than 200 Florida hospitals.(6)
Coincidental (or Strategic?) Solutions
Adding this population growth to the overall loss of physician labor, Florida finds itself in need of local solutions that cannot be solved just by importation of physicians from outside the state. Fortunately, one of the most prescient, if not coincidental, solutions to the looming physician labor shortage and expenses associated with physician attrition is the significant growth of osteopathic medical schools in the United States in recent years. This has been particularly beneficial to the state of Florida.
As of this writing, in the United States there are approximately 157 allopathic (MD-granting) medical schools, with 22,666 first-year students,(7) and 58 osteopathic medical campuses, with 9,775 first year students.(8) So, although there are about one third as many osteopathic campuses as allopathic schools, the number of osteopathic students is almost half as many. Both areas of education are growing, but in the past decade, as a percentage, the growth in osteopathic locations and student matriculants has outpaced allopathic education, and this growth is anticipated to continue.
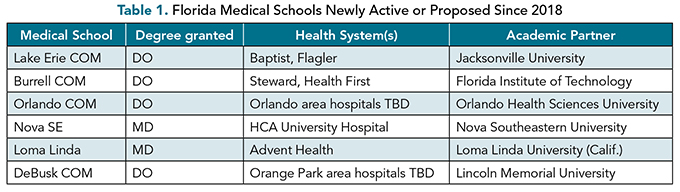
Looking at Florida alone (Table 1), one can see a rapid onset in just 24 months of both new educational sites as well as upcoming proposed programs. Although medical education and subsequent graduate medical education combined usually is drawn out over a period of 7 to 11 years, this growth undoubtedly will help to address the physician labor shortage that is expected in 2034. Other providers (e.g., ARNP, PA) and models of care (e.g., team care, telehealth platforms) also will be required to address the overall anticipated shortage, but as far as hospital productivity goes, physicians remain a key piece of the sustainability models.
Across the United States, large nonacademic hospital systems have embraced the integration of both undergraduate and graduate medical education over the years, with the most widely known being HCA and Kaiser. More recently, smaller, more regional integration examples include proposals of collaboration between Wake Forest University and Atrium Health in North Carolina, the University of Northern Colorado and Banner Health, and Rowan University in New Jersey and Virtua Health. There also is at least one proposal for direct ownership of a college of osteopathy, by Meritus Health in Hagerstown, Maryland. Lastly, in the ambulatory setting, there are a number of proposed partnerships, such as Keck Graduate Institute with LA Care Health Plan, University of Minnesota with CentraCare, and Maryland COM at Morgan State with Baltimore Medical.
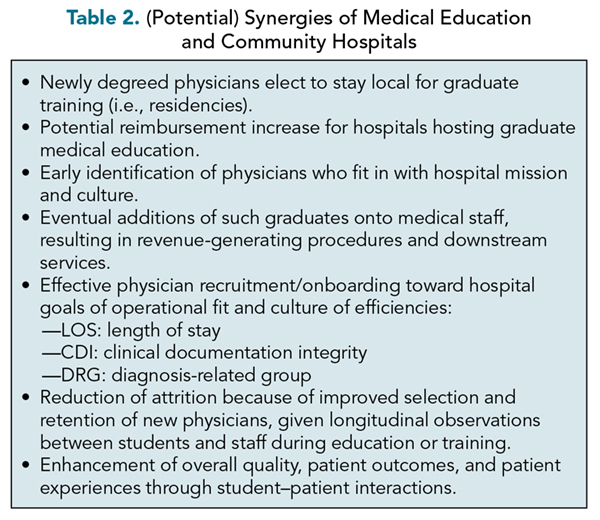
Why is this integration such a timely (if yet unproven) solution? It offers a constructive way to train, recruit, and retain doctors who fit in (culturally or otherwise). Following undergraduate medical education, hospitals can continue to develop the pipeline of talent through graduate medical education. If hospitals are “virgin” with respect to graduate medical education programming, and provided that all requirements and certifications are met, the Accreditation Council of Graduate Medical Education will approve such programming. Such educational programming is funded in a variety of ways, but in no small part CMS is structured to increase payments to hospitals that have residencies, given the “cost” of caring for their Medicare beneficiaries receiving services rendered by residents. If carefully managed, this extra reimbursement stands to be accreditive for the institutions involved. It would be natural, therefore, to combine both undergraduate and graduate medical education at institutions that are attempting to create a longitudinal recruitment and retention strategy. Students who complete their undergraduate and graduate medical education in the same state are highly likely to stay in that state; in Florida that number is 78.8%.(9) Table 2 lists the potential benefits of vertical integration of medical education with community hospitals.
How is This Rapid Expansion Taking Place?
The United States has a long history of replicating and reinforcing the laws of supply and demand. In its simplest incarnation, the forces behind the expansion and the requirements that must be met in order to succeed are notable. Medical education requires the inspection and the approval of one of two accrediting bodies, the Liaison Committee on Medical Education (LCME) or Commission on Osteopathic College Accreditation (COCA). These two bodies are the only pathways relative to medical education recognized by the U.S. Department of Education. The former, LCME, grants certification to confer the degree Doctor of Medicine (MD); the latter, COCA, grants certification to confer the degree Doctor of Osteopathic Medicine (DO). In general, the processes of accreditation are similar; however, the requirements for allopathic education require a significant financial commitment by the hosting academic institution, which can be quite challenging to achieve, or, in some cases, cost prohibitive. Regardless, post-graduate training is now a unified pathway through ACGME. The results of the tests of competency (e.g., USMLE, COMLEX) also are displaying parity across either an allopathic or osteopathic education pathway. The net result is that, regardless of the educational model, physician labor production efforts are becoming nearly indistinguishable from each other.
On the other hand, given that osteopathic schools are more distributive in nature regarding the educational pathway, the osteopathic programs may not always need to set up the same internal infrastructure in order to deliver its content to medical students. This frees up osteopathic programs to move with a bit more agility, and, ultimately, speed “to market.” Added to that is the fact that in our commerce system, structural solutions to face unmet needs and demands often are launched with partners who have access to capital. Institutions of higher education, whether private or public, for profit or not for profit, all have access to capital:
Through philanthropic donations: via endowments, fundraising, ongoing charitable contributions, to name a few;
Through financial institutions: in the form of lending and borrowing in the form of bonds and credit lines;
Through legislation: in the form of tax benefits or distributions); or
Through private capital: in the form of private equity, venture capital, or investment banking, to name a few.
All of these forms of financial support are heavily integrated into higher learning, and all of these bring multiple stakeholders to the table for institutional accountability. Of note, many health systems and, of late, physician employers have the same types of capital structures as with higher learning.
Criticism of Growth
Keeping these structural and financial forces in mind, it is not surprising that the number of osteopathic programs in the United States has increased at a relatively faster pace than the number of allopathic schools. Furthermore, it also is not surprising that some of the DO schools have been backed by the types of financial structures that foster speed to market.
In the face of the intense pressure on U.S. healthcare to meet the needs of its growing and aging population, coupled with the pent-up demand for services that were delayed due to the COVID-19 pandemic’s limitations on access to care, the expansion of the physician labor force comes at a much needed time.
A striking feature of this fortuitous growth in medical education is that there are those who prefer to make divisive statements. Although some of those reporting on the matter present the appearance of fair and balanced reporting,(10) others range from offers of cautionary wisdom to the accreditation bodies to make sure that the principles and standards of medical education are not diluted or influenced by the growth, thereby impacting the educational experiences to the detriment of students, and, ultimately patients, to suggestive statements that impugn the stakeholders of the newer osteopathic schools that have looked for novel capital partners in order to meet the demand.(11) One of the early skeptics of for-profit osteopathic medical school models has publicly recalibrated his position on the matter and is now a proponent of the enterprising manner in which schools can grow to fill the gaps in physician labor.(12,13)
Next Steps
What appears to be missing from words of caution or words of detraction are words that offer a solution. Given the extraordinary pressures on acute care facilities outlined earlier, perhaps it would be more helpful to expand the resources of accreditors in order to meet the growing demand. The growth of such bodies would expand their capability for growth in the physician education sphere (and this extends to residency programs as well) to meet the needs of the healthcare communities under strain and the populations they serve. With the increase in the number of physicians retiring, there exists an available pool of experienced, talented, and smart individuals who could be trained in accreditation and pick up very meaningful work in their nascent transition to new or late careers. It would not be unreasonable for LCME and COCA to continue to seek financial support from a variety of stakeholders to expand their site surveyors and their capacity to manage school proposals, as well as to map out processes that ensure accountability of the supporters of the new schools. Another long-range solution for consideration would be to make it possible for the new medical schools to choose (with ongoing community support) to eventually become foundations for expansion into additional higher learning, such as for nursing and ancillary schools, both of which are desperately needed to fill another labor gap in the U.S. healthcare system.
In the United States, despite its flaws and inadequacies, our way of life is an ongoing experiment in freedoms and protections, checks and balances. Our commerce reflects those principles. The institutions that serve its citizenry can and should be afforded opportunities to meet its needs, especially when circumstances require. Medical schools in the United States, particularly osteopathic institutions, are rapidly turning to creative financial and educational partnership solutions in order to go from conception to groundbreaking to ribbon cutting. The clock is ticking, and the timing is right to support vertical integrations of these expanding medical schools into community hospital settings in order to assist the U.S. healthcare system as much as possible and for the foreseeable future.
References
National Hospital Flash Report: March 2023. KaufmanHall. www.kaufmanhall.com/insights/research-report/national-hospital-flash-report-march-2023 . Accessed March 23, 2023.
Health Forum LLC. Fast Facts on US Hospitals, 2022, AHA Hospital Statistics Infographic. Washington, DC: 2022.
Physicians left their jobs by the hundreds of thousands in 2021. Modern Healthcare. October 20, 2022. www.modernhealthcare.com/physicians/physicians-left-their-jobs-droves-2021-report . Accessed October 20, 2022
IHS Markit Ltd. The Complexities of Physician Supply and Demand: Projections From 2019 to 2034. Washington, DC: AAMC; 2021.
Vintage 2022 national and state population estimates; U.S. Census Bureau 2022. https://www.census.gov/programs-surveys/popest/data/tables.html
Florida Statewide and Regional Physician Workforce Analysis: 2019 to 2035. 2021 Update to Projections of Supply and Demand Prepared for the Safety Net Hospital Alliance of Florida and the Florida Hospital Association; HIS Markit Ltd. https://safetynetsflorida.org/wp-content/uploads/Florida-Physician-Workforce-Analysis.pdf
2022 FACTS: Enrollment, Graduates, and MD-PhD Data; AAMC. www.aamc.org/data-reports/students-residents/data/2022-facts-enrollment-graduates-and-md-phd-data . Accessed October 28, 2022.
Osteopathic Medical School Growth Trends 2011-12 to 2021-22; AACOM. www.aacom.org/become-a-doctor/about-osteopathic-medicine/quick-facts .
2021 State Physician Workforce Data Report. Washington, DC: AAMC; 2021.
Once banned, for-profit medical schools are on the rise again in the U.S. Shots: Health News from NPR. www.npr.org/sections/health-shots/2021/06/07/1002477044/once-banned-for-profit-medical-schools-are-on-the-rise-again-in-the-u-s . Accessed June 7, 2021.
Shireman R. For-profit medical schools—concerns about quality and oversight. N Engl J Med 2022;387:2105-2107. https://doi.org/10.1056/NEJMp2117605
Mychaskiw G. COM accreditation: the Flexner Report revisited [letter]. J Am Osteopath Assoc. 2007;107:246-247,277.
Mychaskiw G. For-profit medical education. JAMA. 2017;318:301.