
Pulmonary embolism (PE) and deep venous thrombosis (DVT) in the postoperative period are significant causes of morbidity and mortality.(1) The Agency for Healthcare Research and Quality (AHRQ) Patient Safety Indicator 12 (PSI-12) focuses on the prevention of postoperative PE and DVT as avoidable causes of patient harm. Retrospective case review identified that the population of patients with orthopedic fractures represented a substantial opportunity for reduction in postoperative PE and DVT. The AHRQ PSI-12 indicator is one of the many publicly reported measures for CMS. The measure also is included in CMS Overall Hospital Quality Star Rating and CMS Hospital Acquired Condition Reduction Program, and is considered a complication for the total hip/total knee arthroplasty patient population for CMS value-based purchasing measure.
Patients at the highest risk for postoperative PE and DVT include those with baseline mobility issues, those with traumatic injury, and those requiring surgical procedures. Early identification of patients at moderate to high risk for developing postoperative PE and DVT is critical to implementation of effective prophylaxis strategies. Delays to operative fixation and withholding chemical or mechanical prophylaxis can be sources of significant patient morbidity and mortality.(2,3)
Fracture alert protocols are critical to mitigate risk and improve patient care. Early patient identification, accelerated surgical clearance, and strict compliance with mechanical and pharmacologic prophylaxis is crucial to avoid postoperative PE and DVT. When combined with enhanced recovery after surgery (ERAS) protocols, prioritized early intervention strategies can lead to a substantial reduction in PSI-12 events.(4,5)
Methods
A retrospective case review determined that the vast majority of cases of postoperative PE and DVT at the study site were related to femoral fracture; no other postoperative PEs or DVTs were found in patients with other orthopedic fractures. All elective orthopedic patients were excluded from the study. The team identified several areas of opportunity, including timely initiation of mechanical prophylaxis, pharmacological prophylaxis for patients not admitted on oral anticoagulation in the preoperative period, and decreasing time to operative fixation. A multidisciplinary team developed a fracture alert protocol. Upon presentation to the emergency department, fracture patients were identified, and a standardized care pathway was initiated. Figure 1 illustrates the fracture alert pathway.

Figure 1. Flowchart illustrating procedure for reducing cases of venous thromboembolism. DVT, deep venous thrombosis; ED, emergency department; OR, operating room; PCP, primary care provider.
At the time of a patient’s admission to the hospital, a DVT risk assessment tool based on the Caprini model was completed.2 When the DVT risk assessment within the EMR admission order set had been completed, the admitting provider was queried to order appropriate pharmacologic prophylaxis, either subcutaneous heparin or low-molecular-weight heparin (LMWH), and/or mechanical prophylaxis. Audits were conducted to ensure risk assessments were calculated appropriately. The orthopedic physician was notified of the fracture by the emergency department to coordinate surgery availability. The hospitalist team evaluated fracture alert patients, providing expedited clearance in less than 12 hours. Current clinical practice guidelines from the American College of Chest Physicians recommend that patients with hip fracture receive administration of LMWH upon admission to hospital, with medication held 12 hours before surgical procedure.(6) To ensure surgery was not delayed, subcutaneous heparin was administered if surgery was scheduled within 12 hours of initial presentation, and LMWH was administered if surgery was scheduled for more than 12 hours after initial presentation, per American Society of Regional Anesthesia and Pain Management anticoagulation guidelines. This allowed for flexibility in the anesthesia care plan and minimization of bleeding.(7) A common practice of withholding preoperative pharmacologic prophylaxis was identified as pervasive among providers. A concern existed for increasing the chance of intraoperative bleeding, which could result in increased transfusion requirements or limitations of the anesthesia care plan. Postoperatively, appropriate pharmacologic prophylaxis was ordered and administered 12 hours after wound closure. Sequential compression devices were applied any time the patient was in bed or chair. Evaluation by a physical therapist and occupational therapist occurred within 24 hours of surgery. When patients were unable to participate in physical therapy, nursing staff initiated an early ambulation protocol. Upon the patient’s discharge from the hospital, the orthopedic team ensured appropriate pharmacologic prophylaxis, and bilateral compression stockings were ordered. Orthopedic and quality care teams monitored compliance with pharmacologic prophylaxis, mechanical prophylaxis, and early ambulation daily following the surgical procedure.
Formal and informal educational sessions were provided to the multidisciplinary team, specifically targeting nursing staff, physicians, and hospital advanced practice providers. This education included presentations to the Surgical Quality Committee and emails to medical staff. All new nursing staff on the surgical unit attended a half-day orthopedic workshop led by the orthopedic clinical nurse specialist (CNS), which included information regarding the fracture alert pathway and their nursing responsibilities in the process. This workshop was scheduled once every quarter to assure all new employees received the information.
Data collection, including reviewing and comparing total number of postoperative PE and DVT cases before and after implementation of procedural and educational changes, was performed. Figure 2 displays multiple interventions in the fracture alert protocol. The study was submitted to the institutional review board (IRB), and it was determined that IRB review and approval was not required.
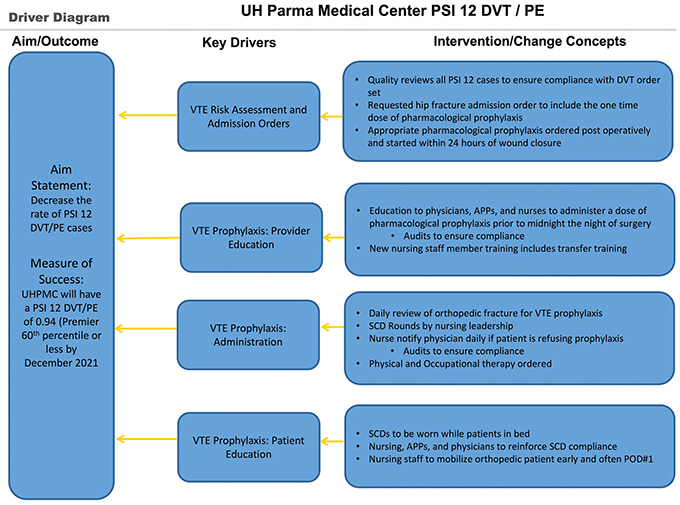
Figure 2. Key drivers for the reduction of venous thromboembolism cases.
Results
In the two-year pre-implementation period, the study site had 8 cases of postoperative PE and DVT out of 162 patients with orthopedic fractures (DRG 480, 481, and 482).(8) After education and implementation of the clinical protocol, postoperative PE and DVT in the orthopedic fracture patients saw a reduction to 0 out of the 482 orthopedic fracture patients in the two years post implementation.
A chi-square analysis was completed to examine the results for statistical significance. Implementation of the clinical protocol led to a statistically significant drop in cases of postoperative PE and DVT at the study site (p <.0001). Table 1 details the results of statistical analysis.

The patient populations were compared for the pre- and post-implementation periods and indexed for patient acuity using American Society of Anesthesiology scoring and case mix index for the orthopedic fracture DRGs 480, 481, and 482, as well as patient age (Table 2).

Data also were obtained and reviewed comparing postoperative blood transfusions pre- and post-implementation of the pharmacologic prophylaxis protocols. There was found to be no increase and a slight reduction in the utilization per case of packed red blood cell (pRBC) transfusions for patients with orthopedic fractures. Specifically, in the pre-implementation period, 59 of 162 (36%) of our patients with orthopedic fractures required pRBC transfusion after surgery. Conversely, 166 of 482 (34%) of the same population required pRBC transfusion after surgery in the post-implementation phase (chi-square analysis p value = .7122).
Limitations
Definitive causation between interventions and results could not be made because the study was observational, rather than a randomized controlled trial. Detailed patient data were limited, and did not include specific age of patients or the presence of preoperative risk factors such as obesity, pathologic fractures, preoperative mobility status, and previous history of DVT or PE.
The current results do not evaluate for the presence of preoperative nonsymptomatic DVT. Another limitation to the results is that we did not compare heparin versus LMWH. The specific anticoagulant used both pre- and postoperatively may have a different rate of efficiency in preventing DVT and PE. The study measures PE and DVTs meeting the PSI-12 definition, and measures events occurring during the index admission.
High turnover rates of staff during the COVID-19 pandemic slowed adoption of the protocols. Continued education was needed to perpetuate this practice change. Surgeon and operating room availability limited the process at times. All-inclusive education of providers was attempted, but was focused on orthopedic surgeons, emergency physicians, and hospitalist physicians.
Discussion
To implement early administration of pharmacologic prophylaxis, collaboration with the emergency medicine team was crucial to ensure the fracture alert pathway was adopted. As soon as the fracture is identified, pages or text messages are sent to all appropriate individuals. After the alert is initiated, direct communication occurs between the trauma coordinator, orthopedic advanced practice provider (APP), and the surgical manager to coordinate surgical timing. The surgical manager then communicates directly with the orthopedic surgeon to schedule the procedure, while the orthopedic APP communicates with the medical provider to ensure prompt medical optimization. If one of these two steps cannot be done within 12 hours, the provider is notified to order venous thromboembolism (VTE) prophylaxis.
Before the implementation of the project, preoperative pharmacologic prophylaxis was withheld in patients with orthopedic fractures due to concern about operative delay and postoperative bleeding. In compliance with American Society of Regional Anesthesia and Pain Medicine guidelines, patients who had a delay in operative fixation were administrated pharmacologic prophylaxis. Partnering with anesthesia providers and other surgical colleagues to help dispel fears of increased bleeding was crucial in the adoption of the preoperative pharmacologic prophylaxis aspect of the protocol. Due to concern regarding potential increased bleeding, transfusion rates were monitored continually to ensure that no increase was noted in blood utilization in the fracture population.
Since the protocol was implemented, all members of the team prioritize getting the patient optimized quickly for surgical intervention.
All components of the Driver diagram were able to be implemented in this protocol. Since the protocol was implemented, all members of the team prioritize getting the patient optimized quickly for surgical intervention. Optimization requires the medical team to see the patient in a timely fashion after admission. The surgical team must ensure room availability with appropriate staffing, and the orthopedic team must be available to evaluate the patient and perform the surgery. Coordination and frequent communication among all teams is essential to ensure patients are taken to surgery in a rapid fashion and/or appropriate interventions are implemented. Consistent collaborative efforts were made by all members of the team to ensure patient optimization, and the protocol was consistently implemented; therefore, no disputes regarding patient management occurred between members of the patient care team.
Substantial effort, led by our chief medical officer, was placed on facilitating communication between physicians and resolving practice inconsistencies. The proactive establishment of periodic touchbases with providers was beneficial in minimizing the number of issues requiring immediate intervention.
Conclusions
After review of postoperative PE and DVT rates and transfusion data, it was concluded that it was safe and effective to give subcutaneous heparin 8 to 12 hours before surgery for patients with orthopedic fractures who were not on oral anticoagulation prior to admission. Collaboration with the multidisciplinary care team to provide safe care was a crucial protocol implementation.
Although this population of patients remains at high risk for postoperative DVT and PE, the initiation of this protocol continues to achieve durable results to achieve zero patient harm. The interventions successfully reduced the rate of postoperative PE and DVT in patients with hip fracture. Changing the culture to ensure that pharmacologic prophylaxis was administered prior to surgery did not increase postoperative blood transfusion rates. Monitoring of intraoperative blood loss as well as other complications, such as postoperative hematomas, should be continued in this patient population.
References
Temgoua MN, Tochie JN, Noubiap JJ, et al. Global incidence and case fatality rate of pulmonary embolism following major surgery: a protocol for a systematic review and meta-analysis of cohort studies. Syst Rev. 2017;6(1):240. https://doi.org/10.1186/s13643-017-0647-8
Cronin M, Dengler N, Krauss ES, et al. Completion of the updated Caprini risk assessment model (2013 Version). Clin Appl Thromb Hemost. 2019;25:107602961983805. https://doi.org/10.1177/1076029619838052
Leer-Salvesen S, Dybvik E, Engesaeter LB, Dahl OE, Gjertsen JE. Low-molecular-weight heparin for hip fracture patients treated with osteosynthesis: should thromboprophylaxis start before or after surgery? An observational study of 45,913 hip fractures reported to the Norwegian Hip Fracture Register. Acta Orthop. 2018;89:615-621. https://doi.org/10.1080/17453674.2018.1519101
Zhao K, Wang Z, Tian S, Hou Z, Chen W, Zhang Y. Incidence of and risk factors for pre-operative deep venous thrombosis in geriatric intertrochanteric fracture patients. Int Orthop. 2021;46:351-359. https://doi.org/10.1007/s00264-021-05215-x
Yoon JY, Kim S, Chang JS, Yoon PW, Kim JW. Venous thromboembolism after delayed surgery for a hip fracture: a retrospective cohort study. Geriatr Gerontol Int. 2020;20:1151-1156. https://doi.org/10.1111/ggi.14055
Kearon C, Akl EA, Comerota AJ, et al. Antithrombotic therapy for VTE disease. In: : Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines [published correction appears in Chest. 2012 Dec;142(6):1698-1704]. Chest. 2012;141(2 Suppl):e419S-e496S. https://doi.org/10.1378/chest.11-2301
Horlocker TT, Vandermeuelen E, Kopp SL, Gogarten W, Leffert LR, Benzon HT. Regional anesthesia in the patient receiving antithrombotic or thrombolytic therapy. Regional Anesthesia and Pain Medicine. 2018;43:263-309. https://doi.org/10.1097/AAP.0000000000000763
2023 DRG List. Updated October 1, 2022. Accessed May 23, 2023. www.icd10data.com/ICD10CM/DRG .