
Abstract:
Primary care is evolving in response to payment reform, changes in the primary care workforce, and development of new models of work emphasizing team care. The role of registered nurses in these new models is being reexamined and reimagined, with increased registered nurse engagement in chart review prior to visits, histories and physicals, preliminary patient assessment, patient education and coaching in ordered care, delivery of care under standardized orders and protocols, transition planning, and care coordination. The business case for employing registered nurses in these new roles has not been fully addressed. This article examines the business case and financial issues in this expansion of practice. Under both fee-for-service and value-based, capitated, or shared saving models of reimbursement, there are strategies for increasing the number of registered nurses in primary care practices, and expanding the engagement of registered nurses that can increase net revenues for primary care practices, even when the costs of the additional staffing are taken into account.
Primary care is evolving in response to payment reform, changes in the primary care workforce, and development of new models of work emphasizing team care. Advanced practice registered nurses (APRNs) are part of this evolution, but in this evolving landscape, the role of RNs who are not APRNs is also being reexamined and reimagined. A growing literature is describing these potential roles and their implementation in healthcare delivery. The business case for employing RNs in these new roles, however, has not been fully assessed. In this paper, I explore the business case and financial issues in expanding the use of RNs in primary care.
Current Staffing for Primary Care
Office-based professional practices make use of a wide-variety of staff, including medical assistants (MAs), licensed practical nurses/licensed vocational nurses (LPNs), and RNs. A 2011 report states that practices preparing to assume the role of a patient-centered medical home employed, on average, 1.4 MAs, 0.3 LPNs, 0.4 RNs, and 0.1 physician assistant for each physician.(1) There is wide variability in the use of office-based primary care staff based on variations in work allocation in practices and number of primary care providers, with some evidence of economies of scale.(2-4)
The roles played by RNs differ from those played by MAs or LPNs. RNs, with their broad training, extensive education in patient assessment and clinical care, and licensed scope of practice, have the potential to play the broadest role. Bielamowicz and Berra,(5) however, report a narrower range of typical activities for RNs and a clear contrast with the role played by MAs and LPNs. RNs were “tied up with incoming patient care triage,” while MAs and LPNs were used to room patients and perform basic administrative tasks.(6)
Roles in traditionally organized primary care practices are driven, in part, by the cost of different categories of personnel. The compensation analytic website salary.com reported that in February 2016, the average salary for a staff RN in outpatient care was $65,412, contrasting with LPNs in outpatient care ($43,397) and MAs ($32,692). These salary differentials encourage common tasks in patient rooming and charting, taking vital signs, checking for allergies, electrocardiograms, stocking supplies and refilling medications, and, where allowed by state law, administration of drugs or vaccines, to devolve in many primary care practices to MAs or LPNs,(7) and minimizing the role of RNs to areas such as triage.(8)
There has been growing recognition of the particular strengths of RNs in a variety of roles in primary care.
There has been growing recognition of the particular strengths of RNs in a variety of roles in primary care. More recently there have been a number of studies examining the roles of RNs specifically in primary care practices.(9-13) These more recent studies identified additional roles that were less common two decades ago (e.g., transitional care, Lean/quality improvement practices, and telehealth) and that specifically enhance new primary care delivery models, including intensive care management, medication reconciliation, direct patient care, and health coaching.
Strategies to Accommodate Increased Engagement of Registered Nurses in Primary Care
As the new models of care have been evolving, primary care has been reimagined as team-based, with expanded roles for the entire healthcare team.(6,8,9,13-20) In these expanded teams, the number of staff per primary care provider is increased.
Increasing the role of RNs in the physician or primary care provider visit to leverage the provider’s time is reflected in the concept of a co-visit. In many primary care practices, MAs room patients, take vital signs, perform some ordered procedures following the physician examination of the patient, and may do some charting of the examination. The co-visit substantially expands this set of tasks, with the RN taking the lead in taking the patient history and doing portions of the physical examination and making a provisional assessment of the patient. After these activities, the physician joins the visit, receives a structured report from the RN, completes the examination, makes or confirms the diagnosis, and prescribes treatment. Nurses often complete the visit by providing additional information to the patient on the treatment and followup and complete the documentation. The service can be billed under one of the standard evaluation and management codes. The primary care provider’s time in direct contact with the patient is reduced, and he or she can complete more billable visits during the same time period. The more extended time spent with the patient can also result in a legitimate increase in the time and intensity of the visit, justifying coding the visit as a more intensive visit with a higher payment level.
A second strategy for expanding billable services is a nurse-only visit. If this is done for an established patient, the physician is in the facility, and a standard procedure has been established, the practice may be able to bill for a nurse-only visit under billing code 99211.
Examples of services provided by RNs that can be billed under code 99211 include immunizations, prescription refills and adjustment of dosages of specific drugs such as insulin based on laboratory or clinical findings, other diabetes management activities, and treatment of specific infections such as Streptococcus or urinary tract infections in uncomplicated patients. As with co-visits, a protocol embedded in a standing order is essential for allowing RNs to conduct these services without the patient seeing a primary care provider.(21)
Other billable options for nurse-only visits incident-to physician services include Medicare’s Annual Wellness Visit(22) and Medicare chronic care management services.
The third element of the expansion of RN roles in primary care is increasing RN engagement in services that may not be directly billable, adding to the FTEs without obvious fee-for-service (FFS) reimbursement. Examples include RN-led new patient visits and RN-led chronic care management visits not billable under current contracts or rules. In an environment in which practices are bearing the risk because they have accepted capitation or there are value-based penalties for higher-cost patients, the costs of these unreimbursed services may be recovered through other savings. They also can be revenue enhancing with bonuses for pay-for-performance and other payment models built on improved patient outcome, which can be very generous.(23,24)
The Business Case for an Expanded Role for Registered Nurses in Primary Care
The business case question is whether the additional costs of staffing can be offset, either with higher revenues or with cost reductions in other areas. The answer differs depending on whether the practice is operating under a fee-for-service revenue model, a capitated model, or other value-based purchasing model. Practices increasingly operate under multiple models of payment and may tailor services provided depending on the financial incentives. For example, they may offer case management services to all patients, but aggressively promote these for patients seen under risk contracts. Similarly, they may focus hospital transition services intended to reduce readmissions on patients under capitation or shared savings contracts such as Accountable Care Organization (ACO) agreements.
Fee for Service
In an FFS environment, the cost of increased staffing has to be supported by increased volume and higher billings. These increases could come from increased productivity through co-visits, increased visit intensity justifying a higher billing code, or increased billings from nurse-only visits, wellness visits, or care coordination. For example, as noted earlier, the average salary for an RN in outpatient care was $65,412. If fringe benefits and related costs are 30% (approximately the level reported on salary.com), the cost of adding one FTE RN to a practice would be approximately $85,000. The average Medicare payment in 2013 for billing code 99214, a moderate (typically 25 minute) evaluation and management visit for an established patient, is $106.83; $72.81 for billing code 99213, a low-intensity 15-minute visit for an established patient; and $20.41 for billing code 99211, the code most frequently used for an RN-only visit. Assuming a 220-day work year (allowing for vacations, holidays, and some in-service training and related activities), the salary and benefits would be recovered from a daily average of an additional 3.6 moderate-intensity visits, 5.3 low-intensity visits, or 18.9 nurse-only 99211 visits.
The experiences of two large primary care organizations illustrate the revenue gains that can be realized from the expanded use of RNs in an FFS environment.
Clinica Family Health
Clinica Family Health, in Lafayette, Colorado, tested a co-visit model in 2014.(25) It modified its primary care provider scheduling to eliminate double booking but provided for one to two co-visits for every two standard visits.
The Clinica staffing model is built around a medical pod, serving approximately 3600 patients. Under its original model, a typical pod had three FTE primary care providers (i.e., MDs, DOs, APRNs, physician assistants), 1.24 MAs per FTE primary care provider (or ~3.7/pod), and 1.0 RN. In the tested model, the number of RNs was increased to three per pod, and the number of MAs was increased slightly, to four per pod, to accommodate the increased number of visits. Roles within the pod and clinics also were changed. Phone triage was shifted off the pod, with nurses rotating into triage. Triage declined as more patients were accommodated with same-day visits. In the pod, one nurse provided traditional RN services such as wound care, patient education, case management, and monitoring visits for patients taking warfarin. The other two nurses conducted co-visits. At the annual national salaries, the cost of this additional staffing would be approximately $195,000. Per-visit payment averaged approximately $125/visit, with approximately $25 for supplies per visit. With net revenue per visit of $100, the additional staffing costs could be covered by 1950 visits.
Table 1 presents the data from Clinica Family Health, contrasting staffing under its original pod model with the revised staffing to allow for an expansion of co-visits. Table 2 presents the estimated change in the number of visits and the revenue and expenses associated with that expansion. The 6059 additional visits, approximately two per day per primary care provider, and approximately six co-visits per day per nurse, expand visit capacity by 23% and generate a surplus over expenses, taking labor costs, additional direct costs of supplies, and training into account. The break-even number of visits is 1.53 additional billed visits per primary care provider per day, a number that can be accommodated into the visit grid used by Clinica Family Health under the co-visit expansion model. This model and business case analysis is predicated on there being sufficient demand for same-day visits that are being triaged to later time periods.


Under this model, employees report improved satisfaction and work/life balance, and patient satisfaction with the nurse co-visits was higher than the baseline for provider visits.(25)
Mercy Clinics
Mercy Clinics, Inc., of Des Moines, Iowa, is a 150-physician multisite group practice, with 70% of the physicians in primary care. It has expanded the use of what it calls “health coaches” in a variety of ways in pre- and inter-visit work. Although the initial health coach model envisioned RNs, LPNs, and MAs potentially playing these roles, as the clinic has gained experienced in using health coaches, almost all of them now are RNs.
The coaches work with primary care providers and patients to provide medical home and coordination services, review charts and disease directory data in the clinic to identify patients needing additional care or tests, and identify patients not meeting clinic-level quality performance goals. They are actively involved in patient education.(26-28)
The coaches play significant roles in pre-visit, visit, and post-visit activities. The pre-visit work is a chart review in preparation for the visit. It identifies specific services and follow-up that are noted on a worksheet attached to the chart prior to the visit, and allows for preordering of tests to be conducted during the visit using standing order sets. Other needed preventive services such as mammograms and colonoscopies can also be flagged in the pre-visit chart review. Coaches increase the number of patient visits by doing reminder calls. The pre-visit workup also has ensured more complete care, enabling Mercy Clinics to obtain pay-for-performance payments based on process-of-care measures such as the proportion of patients receiving screening.
During visits, as in a co-visit, the initial history and physical may be taken by the RN health coach. For established patients with chronic conditions, this includes a discussion of adherence to medications and other treatments. Senior clinicians at Mercy Clinics commented in interviews that nurses were more effective than physicians in eliciting information on adherence and problems in following the treatment plans. Coaches also meet with patients after they see their primary care practitioner to discuss the treatment plan and how it will be implemented. The nurses and coaches have more time for these discussions than the primary care practitioners.
Coaches also may follow up when patients are referred to non–Mercy Clinics specialists, to make appointments, follow up with patients immediately after appointments, and proactively offer to schedule any recommended imaging or other follow-up services ordered with Mercy Clinic facilities, retaining the revenue from those ancillary services.
Coaches increase the number of patient visits by doing reminder calls.
This set of health coach activities results in increased visits, increased proportion of visits at a higher visit level, and increased laboratory and imaging services, as well as preventive services such as vaccinations for flu, shingles, tetanus, and pneumonia.
Mercy Clinics also uses RNs in nurse-only visits. It has limited the use of 99211 visits, in part because of concerns over documenting compliance with the “incident-to” rules, but uses them for such services as Coumadin clinics to monitor and adjust doses using standing orders. Mercy Clinics has also made extensive use of nurses in wellness visits, which, under the regulations, can be delegated to RNs under standing orders.
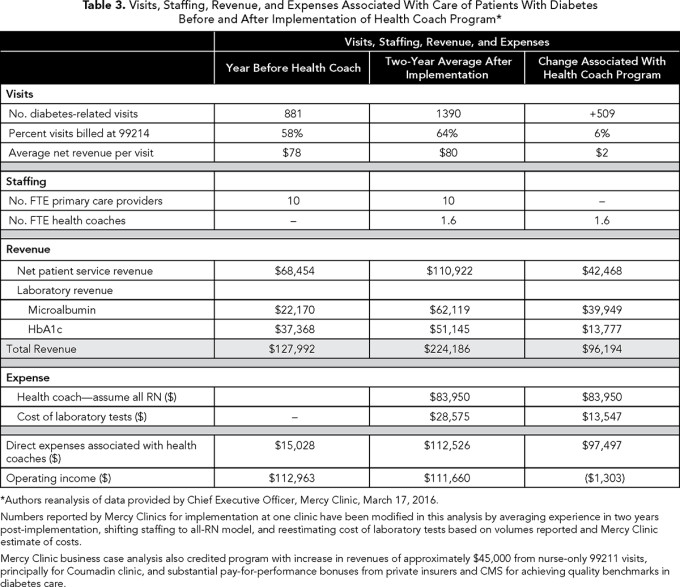
Mercy Clinics has not conducted a full business case analysis of health coaches, but partial analysis of diabetes care has encouraged it to maintain and expand the role in a fee-for-service environment (Table 3). After introducing the equivalent of 1.6 FTE health coaches into a 10-provider primary care clinic, it increased the number of visits for diabetes-related care, increased the proportion of visits billed at the 99214 level, and increased revenue from laboratory services associated with diabetes monitoring for Hb1Ac and microalbumin. With just these services considered and with the 1.6 FTE health coaches costed at RN salaries and benefits, the clinic nearly breaks even. When additional services associated with the health coaches are considered (e.g., nurse-only Coumadin clinic visits, estimated at $45,000 in revenue; increased primary care provider productivity, allowing for more visits per provider, estimated conservatively at $15,000); identification of additional appropriate services for patients who do not have diabetes), the health coach model generates a net profit for the clinics.
Mercy Clinics also has estimated that nurses can potentially conduct eight wellness visits per day, although usually only six per day are scheduled. Using national-level nursing salaries plus benefits, breakeven to cover salary and benefits would be realized at a rate of three visits per day, leaving approximately half of their time for the RN health coach to carry out other activities, revenue-generating or otherwise.
This analysis does not take into account pay-for-performance bonus payments from payers for achieving annual process performance standards along metrics such as the percentage of patients with diabetes receiving HbA1c screening or eye examinations. These bonus payments can be substantial, making the business case even stronger.
Based on its experience, Mercy Clinics is expanding health coach staffing from the approximately one coach per five primary care physicians that was the basis of the partial business case analysis of diabetes presented above.
Alternative Payment Models
We are in a period of changing payment, moving from fee-for-service to other forms of value payment or shifting risk from payers to providers. In addition to performance-based pay-for-performance bonuses and penalties, there is increased use of capitation, bundled payment, and shared savings models such as ACOs. Incentives and business case considerations under these systems differ from those under fee-for-service, with the costs of additional RNs needing to be offset by savings elsewhere.
One opportunity is to expand primary care capacity at a lower cost than hiring additional primary care providers. The Clinica Family Clinic experience offers some insight into this. While the co-visit model was developed to ease high workloads and reduce delays in appointments, it achieved a 23% expansion of visit capacity and a net positive cash flow for the clinic. The breakeven point of an additional 1.53 visits per primary care provider per day represented a 17% expansion of capacity.
Other opportunities involve offsetting the additional cost of primary care practice or additional RNs with savings in other services. The biggest opportunities for savings involve reduced hospitalizations and rehospitalizations, achieved through active care coordination and transition planning, and reduced emergency department use
While models for an increased role of RNs in ACOs have been described,(11) there has been no overall economic evaluation of these models. The efforts by Mercy Clinics to adapt its health coach model to an ACO environment of shared savings suggests several partial business case analyses that can guide planning for expanded use of RNs under these types of payment.
Mercy Clinics’ analysis of its cost-sharing opportunities suggested substantial gains if emergency department use could be reduced by 30% and hospital admissions, including readmissions, reduced by 12%. Its modeling included an increase in primary care visits of 30%, suggesting a substantial role for making care available in lieu of emergency departments, and increased care coordination services. Within this planning framework, Mercy Clinics’ strategy is to segment patient population by health risk, with healthy or low-risk patients receiving appropriate preventive health services and improved access for acute care; stable chronically ill patients receiving targeted intensive services; and high-risk chronically ill patients intensively managed.
In this system, the role of health coaches shifts. Mercy Clinics has hired three FTE transition coaches for post-hospital care for an ACO population of approximately 60,000 patients, at a cost of approximately $200,000. Mercy Clinics estimated that the cost of a readmission is approximately $10,000. Under a fully capitated system, the cost of the program would be recovered with a reduction of 20 readmissions, and under a 50% shared saving program, 40 readmissions. At the national hospital admission rate, the Mercy Clinics’ ACO population would have 6800 hospital admissions per year, with 5900 index admissions and 900 readmissions. Reducing readmissions by 40 would reduce the readmission rate by less than one percentage point, and Mercy Clinics believes it can reduce readmissions by three percentage points, generating substantial revenue in excess of break even.
A second change in the health coaching model for ACO patients involves coaches proactively initiating assistance to patients in implementing self-management services and increased coordination and transitional care services. Although their average cost per member per month is approximately $400, patients with multiple dominant or moderate chronic conditions (approximately 15% of its patients) cost $950 per member per month, and patients with more extensive chronic conditions (~1% of its patients) cost $2300 per member per month. It anticipates assigning approximately 50 high-risk patients to each health coach, although this would not be the sole work of the health coaches working with these patients. If the patient mix of these patients matched the overall mix in the ACO, the total projected annual spending for these 50 patients would be approximately $620,000. As noted earlier, the salary and benefits of a health coach at Mercy Clinics come to approximately $60,000. A 10% reduction in health spending on these patients through more effective care coordination and reduced hospitalization would fully pay for the coach, not considering other services and savings achieved by the coaches with other patients, or other value-based bonuses for achieving targets for patient-reported experience, population-based immunization, screening and treatment targets, or readmission or admission rates. A 5% reduction would cover half the cost of the coach.
Fully integrated business case analysis for capitated or shared savings programs can be difficult, because there are multiple areas of costs and possible savings plus specific bonus and pay-for-performance goals that create a complicated planning environment. This analysis suggests that organizations can make progress toward assessing the value of interventions by identifying specific targets for improvement (e.g., readmission rates, hospitalization rates, emergency room use), the magnitude of improvement that can realistically be achieved; the cost return or revenue associated with those improvements; and, based on this, the costs for a program that would make pursuing those goals appropriate for the organization. Experience with medical homes and patient-centered primary care suggests the interventions to achieve improvement involve increased transition planning and care coordination, areas in which nurses excel.
Conclusion
Because of cost considerations, RN employment in primary care has been limited, with a focus on triage and supervision of less trained staff such as LPNs and MAs, and limited utilization of RN skills in assessment, treatment, and patient engagement and mobilization. The changing demands on primary care, shortage of primary care providers, and growth of patient-centered models and team-based primary care have increased demands for the RN competencies in assessment, treatment, communication, patient engagement, and education. Models for achieving increased engagement of RNs in primary care, tapping their expertise, and reducing the demands on primary care providers are being developed. These include such mechanisms as RN co-visits, nurse-only visits using standing orders, and increased roles for RNs in care coordination, telemedicine, patient education, and health coaching.
Increasing RN involvement in these activities will require increasing the ratio of RNs to primary care providers from the current average of approximately 0.4 up to 1.0 per primary care provider. This will add to the direct cost of these practices, but there are ways to implement these models that can fully offset these costs and increase net revenues of practices, creating a positive business case for an expanded RN role in primary care. In a fee-for-service environment, increased billable services through co-visits and nurse-only visits can pay for themselves. In a capitated environment the additional costs will have to be offset by reduced use of other services such as emergency departments and inpatient care. Business case analysis of specific interventions such as those targeted at reduced hospital readmissions or at reducing admission risk for high-risk individuals with chronic conditions indicate that increased engagement of nurses in these specific programs can improve care and not only recoup the costs but generate additional net revenue for primary care practices.
Acknowledgement: Funding was provided by Josiah Macy Jr. Foundation. The author wishes to thank Ellen Marie Whelan, Diana Mason, Thomas Bodenheimer, and Stephen Shoenbaum for their review of an earlier version of this paper.
References
Berra A. Benchmarking clinical support staff in primary care sites. The Blueprint Blog. 2011. www.advisory.com/research/health-care-advisory-board/blogs/the-blueprint/2011/07/benchmarking-clinical-support-staff-in-primary-care-sites. Accessed March 4, 2016.
Peikes DN, Reid RJ, Day TJ, et al. Staffing patterns of primary care practices in the comprehensive primary care initiative. Ann Fam Med. 2014;12:142-149.
Aita V, Dodendorf DM, Lebsack JA, Tallia AF, Crabtree BF. Patient care staffing patterns and roles in community-based family practices. J Fam Pract. 2001;50:889.
Reeves CS. How many staff members do you need? Fam Pract Manag. 2002;9(8):45-49.
Hackbarth DP, Haas SA, Kavanagh JA, Vlasses F. Dimensions of the staff nurse role in ambulatory care: Part I—Methodology and analysis of data on current staff nurse practice. Nursing Economic$. 1995;13(2):89-97.
Bielamowicz L, Berra A. Benchmarking medical home staffing models: learning from The Advisory Board’s Medical Home Project. 2011; www.ehcca.com/presentations/medhomesummit3/berra_ms3.pdf . Accessed March 12, 2016, 2016.
Eldridge CW. Expanding Roles of Medical Assistants in the Patient Centered Medical Home. Portland, ME: Muskie School of Public Service; 2013.
Ladden MD, Bodenheimer T, Fishman NW, et al. The emerging primary care workforce: preliminary observations from the primary care team: learning from effective ambulatory practices project. Acad Med. 2013;88:1830-1834.
Lamb G, Newhouse R, Beverly C, et al. Policy agenda for nurse-led care coordination. Nursing Outlook. 2015;63:521-530.
Leasure EL, Jones RR, Meade LB, et al. There is no “i” in teamwork in the patient-centered medical home: defining teamwork competencies for academic practice. Acad Med. 2013;88:585-592.
Pittman P, Forrest E. The changing roles of registered nurses in Pioneer Accountable Care Organizations. Nursing Outlook. 2015;63:554-565.
Sinsky CA, Sinsky TA, Althaus D, Tranel J, Thiltgen M. Practice profile. “Core teams”: nurse-physician partnerships provide patient-centered care at an Iowa practice. Health affairs (Project Hope). 2010;29:966-968.
Smolowitz J, Speakman E, Wojnar D, et al. Role of the registered nurse in primary health care: meeting health care needs in the 21st century. Nursing Outlook. 2015;63(2):130-136.
American Academy of Ambulatory Care Nursing. American Academy of Ambulatory Care Nursing Position Paper: The Role of the Registered Nurse In Ambulatory Care. www.aaacn.org/sites/default/files/documents/PositionPaper.pdf. Pitman, NJ: American Academy of Ambulatory Care Nursing; 2012.
Bodenheimer T. Building Teams in Primary Care: 15 Case Studies. Oakland, CA: California HealthCare Foundation; July, 2007.
Bodenheimer T. Building Teams in Primary Care: Lessons Learned. Oakland, CA: California HealthCare Foundation; July, 2007.
Bodenheimer T, Laing BY. The teamlet model of primary care. Ann Fam Med. 2007;5:457-461.
Doherty RB, Crowley RA. Principles supporting dynamic clinical care teams: an American College of Physicians position paper. Ann Intern Med. 2013;159:620-626.
Korda H, Eldridge GN. ACOs, PCMHs, and health care reform: nursing’s next frontier? Policy, Politics & Nursing Practice. 2011;12(2):100-103.
Swan BA, Haas SA. Health care reform: current updates and future initiatives for ambulatory care nursing. Nursing Economic$. 2011;29:331-334.
Bodenheimer T, Bauer L, Olayiwola JN, Syer S. RN Role Reimagined: How Empowering Registered Nurses Can Improve Primary Care. Oakland, CA: California HealthCare Foundation; August, 2015.
Swieskowski D, Engelbrecht A, O’Shea N, Piehl D. Scope of practice. Iowa Med. 2014;104(3):14-17.
Haas SA, Swan BA. Developing the value proposition for the role of the registered nurse in care coordination and transition management in ambulatory care settings. Nursing Economic$. 2014;32(2):70-79.
Joo JY, Huber DL. An integrative review of nurse-led community-based case management effectiveness. International Nursing Review. 2014;61(1):14-24.
Funk KA, Davis M. Enhancing the role of the nurse in primary care: The RN “co-visit” model. J Gen Intern Med. 2015;30:1871-1873.
Swieskowski D. Office-based health coaches: creating healthier communities. Group Practice Journal. 2008;57(2):41-45.
Mercy Clinics: The Medical Home. Group Practice Journal. 2008; 57(4):13-17.
Health Coaches Transform Care Delivery: Part 2: 2008 AMGA Acclaim Award Recipient. Group Practice Journal. 2009;58(2):16-23.
Topics
Environmental Influences
Economics
Quality Improvement
Related
Reducing Clinical Variation Through Interdisciplinary Leadership: A Field Report from a Large Academic Medical Center3 Medical Routines That Older People May Not NeedThe Collaboration Imperative: Why Healthcare Executives Must Unite Against an Existential Threat